Lexicon Pharmaceuticals, The Woodlands, TX, USA.
Diabetes Metab Syndr Obes. 2015 Feb 26;8:121-7. doi: 10.2147/DMSO.S76342. eCollection 2015.
Oral agents are needed that improve glycemic control without increasing hypoglycemic events in patients with type 1 diabetes (T1D). Sotagliflozin may meet this need, because this compound lowers blood glucose through the insulin-independent mechanisms of inhibiting kidney SGLT2 and intestinal SGLT1. We examined the effect of sotagliflozin on glycemic control and rate of hypoglycemia measurements in T1D mice maintained on a low daily insulin dose, and compared these results to those from mice maintained in better glycemic control with a higher daily insulin dose alone.
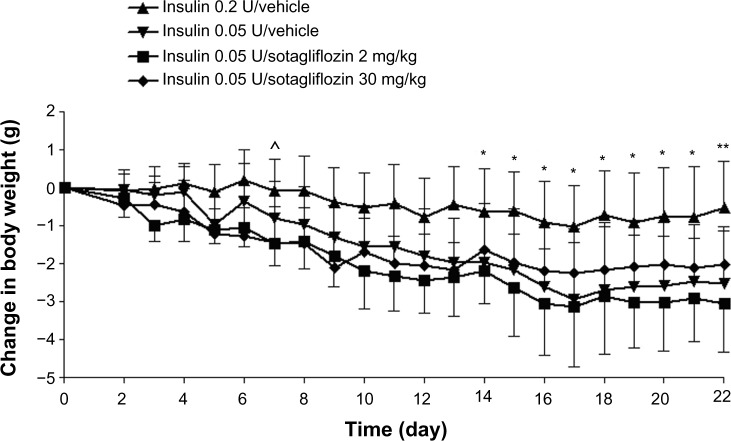
Nonobese diabetes-prone mice with cyclophosphamide-induced T1D were randomized to receive one of four daily treatments: 0.2 U insulin/vehicle, 0.05 U insulin/vehicle, 0.05 U insulin/2 mg/kg sotagliflozin or 0.05 U insulin/30 mg/kg sotagliflozin. Insulin was delivered subcutaneously by micro-osmotic pump; the day after pump implantation, mice received their first of 22 once-daily oral doses of sotagliflozin or vehicle. Glycemic control was monitored by measuring fed blood glucose and hemoglobin A1c levels.
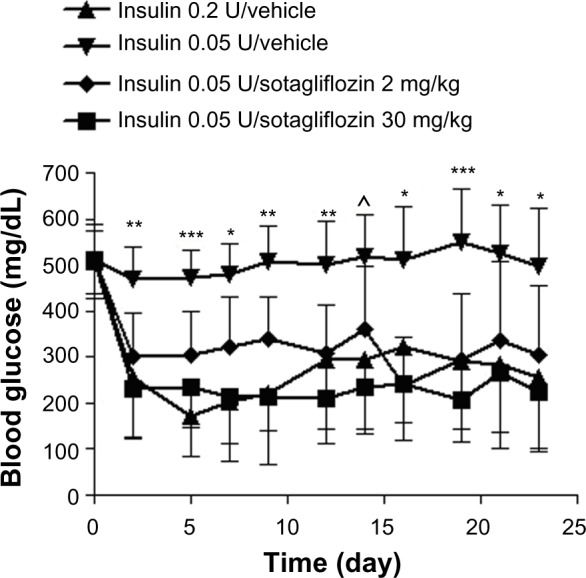
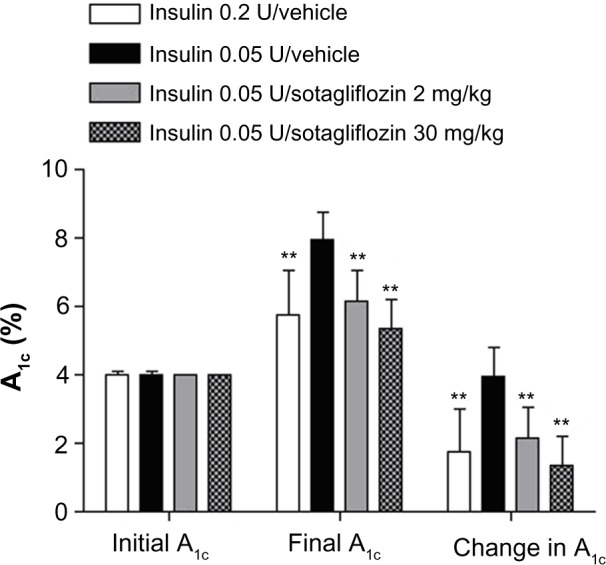
Blood glucose levels decreased rapidly and comparably in the 0.05 U insulin/sotagliflozin-treated groups and the 0.2 U insulin/vehicle group compared to the 0.05 U insulin/vehicle group, which had significantly higher levels than the other three groups from day 2 through day 23. A1c levels were also significantly higher in the 0.05 U insulin/vehicle group compared to the other three groups on day 23. Importantly, the 0.2 U insulin/vehicle group had, out of 100 blood glucose measurements, 13 that were <70 mg/dL compared to one of 290 for the other three groups combined.
Sotagliflozin significantly improved glycemic control, without increasing the rate of hypoglycemia measurements, in diabetic mice maintained on a low insulin dose. This sotagliflozin-mediated improvement in glycemic control was comparable to that achieved by raising the insulin dose alone, but was not accompanied by the increased rate of hypoglycemia measurements observed with the higher insulin dose.
需要有一种口服药物,既能改善 1 型糖尿病(T1D)患者的血糖控制,又不会增加低血糖事件。索格列净可能满足这一需求,因为这种化合物通过抑制肾脏 SGLT2 和肠道 SGLT1 的胰岛素非依赖性机制降低血糖。我们研究了索格列净对接受低剂量胰岛素维持治疗的 T1D 小鼠血糖控制和低血糖测量率的影响,并将这些结果与单独接受高剂量胰岛素维持治疗的血糖控制更好的小鼠的结果进行了比较。
非肥胖糖尿病易感(NOD)小鼠经环磷酰胺诱导发生 T1D 后,随机接受以下四种每日治疗之一:0.2U 胰岛素/载体、0.05U 胰岛素/载体、0.05U 胰岛素/2mg/kg 索格列净或 0.05U 胰岛素/30mg/kg 索格列净。胰岛素通过微渗透泵皮下给药;泵植入后的第二天,小鼠接受第一次 22 次每日一次的索格列净或载体口服剂量。通过测量进食后血糖和血红蛋白 A1c 水平监测血糖控制。
与 0.05U 胰岛素/载体组相比,0.05U 胰岛素/索格列净治疗组和 0.2U 胰岛素/载体组的血糖水平下降迅速且相似,而 0.05U 胰岛素/载体组的血糖水平显著高于其他三组从第 2 天到第 23 天。与其他三组相比,第 23 天,0.05U 胰岛素/载体组的 A1c 水平也显著升高。重要的是,在 100 次血糖测量中,0.2U 胰岛素/载体组有 13 次<70mg/dL,而其他三组的总和为 290 次。
在接受低剂量胰岛素维持治疗的糖尿病小鼠中,索格列净显著改善了血糖控制,而不增加低血糖测量率。这种索格列净介导的血糖控制改善与单独提高胰岛素剂量相当,但没有伴随更高胰岛素剂量观察到的低血糖测量率增加。