Lazer Tal, Dar Shir, Shlush Ekaterina, Al Kudmani Basheer S, Quach Kevin, Sojecki Agata, Glass Karen, Sharma Prati, Baratz Ari, Librach Clifford L
CReATe Fertility Centre, 790 Bay Street, Suite 1100, Toronto, ON, Canada M5G 1N8 ; Department of Obstetrics & Gynecology, University of Toronto, Toronto, ON, Canada M5S 2J7.
CReATe Fertility Centre, 790 Bay Street, Suite 1100, Toronto, ON, Canada M5G 1N8.
Int J Reprod Med. 2014;2014:581451. doi: 10.1155/2014/581451. Epub 2014 Oct 1.
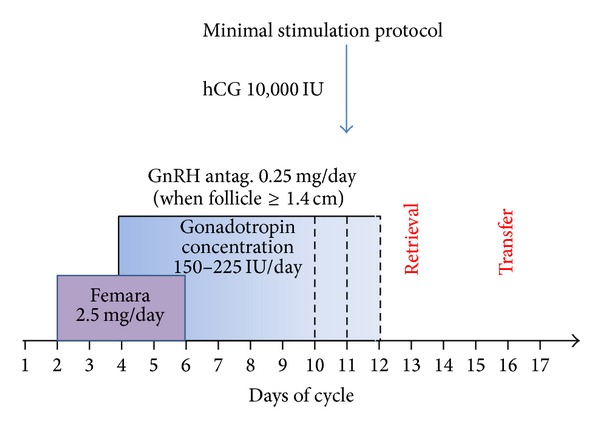
We examined whether treatment with minimum-dose stimulation (MS) protocol enhances clinical pregnancy rates compared to high-dose stimulation (HS) protocol. A retrospective cohort study was performed comparing IVF and pregnancy outcomes between MS and HS gonadotropin-antagonist protocol for patients with poor ovarian reserve (POR). Inclusion criteria included patients with an anti-Müllerian hormone (AMH) ≤8 pmol/L and/or antral follicle count (AFC) ≤5 on days 2-3 of the cycle. Patients from 2008 exclusively had a HS protocol treatment, while patients in 2010 had treatment with a MS protocol exclusively. The MS protocol involved letrozole at 2.5 mg over 5 days, starting from day 2, overlapping with gonadotropins, starting from the third day of letrozole at 150 units daily. GnRH antagonist was introduced once one or more follicles reached 14 mm or larger. The HS group received gonadotropins (≥300 IU/day) throughout their antagonist cycle. Clinical pregnancy rate was significantly higher in the MS protocol compared to the HS protocol (P = 0.007). Furthermore, the live birth rate was significantly higher in the MS group compare to the HS group (P = 0.034). In conclusion, the MS IVF protocol is less expensive (lower gonadotropin dosage) and resulted in a higher clinical pregnancy rate and live birth rate than a HS protocol for poor responders.
我们研究了与高剂量刺激(HS)方案相比,最低剂量刺激(MS)方案治疗是否能提高临床妊娠率。进行了一项回顾性队列研究,比较了卵巢储备功能低下(POR)患者在MS和HS促性腺激素拮抗剂方案下的体外受精(IVF)和妊娠结局。纳入标准包括在月经周期第2 - 3天抗苗勒管激素(AMH)≤8 pmol/L和/或窦卵泡计数(AFC)≤5的患者。2008年的患者仅接受HS方案治疗,而2010年的患者仅接受MS方案治疗。MS方案包括从第2天开始,连续5天服用2.5 mg来曲唑,与促性腺激素重叠,从服用来曲唑的第3天开始,每天150单位。一旦一个或多个卵泡达到14 mm或更大,就开始使用促性腺激素释放激素(GnRH)拮抗剂。HS组在整个拮抗剂周期中接受促性腺激素(≥300 IU/天)治疗。与HS方案相比,MS方案的临床妊娠率显著更高(P = 0.007)。此外,与HS组相比,MS组的活产率显著更高(P = 0.034)。总之,对于反应不良者,MS体外受精方案成本更低(促性腺激素剂量更低),且临床妊娠率和活产率高于HS方案。