Anselmino Matteo, Scarsoglio Stefania, Camporeale Carlo, Saglietto Andrea, Gaita Fiorenzo, Ridolfi Luca
Division of Cardiology, Department of Medical Sciences, "Città della Salute e della Scienza" Hospital, University of Turin, Turin, Italy.
DIMEAS -Department of Mechanical and Aerospace Engineering-, Politecnico di Torino, Turin, Italy.
PLoS One. 2015 Mar 12;10(3):e0119868. doi: 10.1371/journal.pone.0119868. eCollection 2015.
Despite the routine prescription of rate control therapy for atrial fibrillation (AF), clinical evidence demonstrating a heart rate target is lacking. Aim of the present study was to run a mathematical model simulating AF episodes with a different heart rate (HR) to predict hemodynamic parameters for each situation.
The lumped model, representing the pumping heart together with systemic and pulmonary circuits, was run to simulate AF with HR of 50, 70, 90, 110 and 130 bpm, respectively.
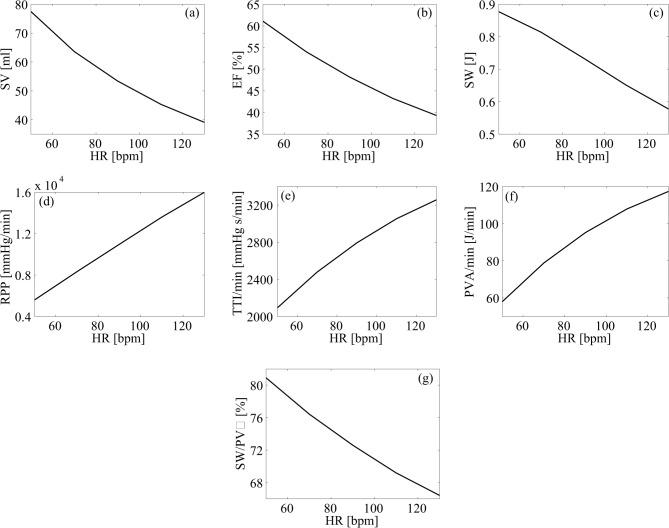
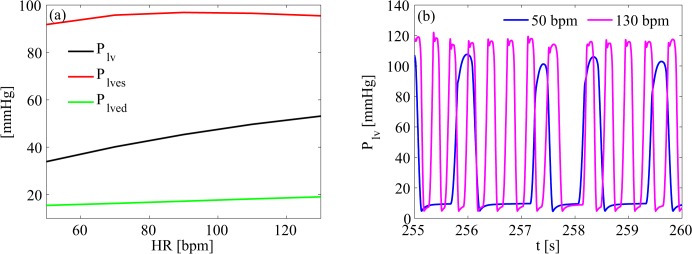
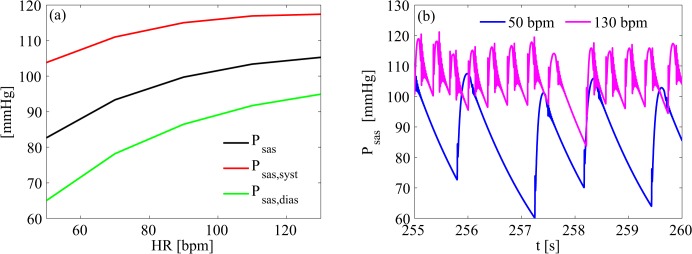
Left ventricular pressure increased by 57%, from 33.92±37.56 mmHg to 53.15±47.56 mmHg, and mean systemic arterial pressure increased by 27%, from 82.66±14.04 mmHg to 105.3±7.6 mmHg, at the 50 and 130 bpm simulations, respectively. Stroke volume (from 77.45±8.50 to 39.09±8.08 mL), ejection fraction (from 61.10±4.40 to 39.32±5.42%) and stroke work (SW, from 0.88±0.04 to 0.58±0.09 J) decreased by 50, 36 and 34%, at the 50 and 130 bpm simulations, respectively. In addition, oxygen consumption indexes (rate pressure product - RPP, tension time index per minute - TTI/min, and pressure volume area per minute - PVA/min) increased from the 50 to the 130 bpm simulation, respectively, by 186% (from 5598±1939 to 15995±3219 mmHg/min), 56% (from 2094±265 to 3257±301 mmHg s/min) and 102% (from 57.99±17.90 to 117.4±26.0 J/min). In fact, left ventricular efficiency (SW/PVA) decreased from 80.91±2.91% at 50 bpm to 66.43±3.72% at the 130 bpm HR simulation.
Awaiting compulsory direct clinical evidences, the present mathematical model suggests that lower HRs during permanent AF relates to improved hemodynamic parameters, cardiac efficiency, and lower oxygen consumption.
尽管心房颤动(AF)的心率控制治疗已常规应用,但缺乏证明心率目标的临床证据。本研究的目的是运行一个数学模型,模拟不同心率(HR)的房颤发作,以预测每种情况下的血流动力学参数。
采用集总模型,该模型代表了心脏泵血以及体循环和肺循环,分别以50、70、90、110和130次/分钟的心率模拟房颤。
在50次/分钟和130次/分钟的模拟中,左心室压力分别从33.92±37.56 mmHg增加到53.15±47.56 mmHg,增加了57%,平均体循环动脉压从82.66±14.04 mmHg增加到105.3±7.6 mmHg,增加了27%。每搏输出量(从77.45±8.50降至39.09±8.08 mL)、射血分数(从61.10±4.40降至39.32±5.42%)和每搏功(SW,从0.88±0.04降至0.58±0.09 J)在50次/分钟和130次/分钟的模拟中分别下降了50%、36%和34%。此外,氧消耗指数(心率血压乘积 - RPP、每分钟张力时间指数 - TTI/min和每分钟压力容积面积 - PVA/min)在从50次/分钟到130次/分钟的模拟中分别增加了186%(从5598±1939升至15995±3219 mmHg/min)、56%(从2094±265升至3257±301 mmHg s/min)和102%(从57.99±17.90升至117.4±26.0 J/min)。实际上,左心室效率(SW/PVA)从50次/分钟时的80.91±2.91%降至130次/分钟心率模拟时的66.43±3.72%。
在等待强制性直接临床证据期间,本数学模型表明,持续性房颤期间较低的心率与改善的血流动力学参数、心脏效率和较低的氧消耗有关。