Mony Prem K, Varghese Beena, Thomas Tinku
Division of Epidemiology, Biostatistics & Population Health, St John's Research Institute, Bangalore, Karnataka, India.
Division of Epidemiology, Biostatistics & Population Health, St John's Research Institute, Bangalore, Karnataka, India Public Health Foundation of India, New Delhi, India.
BMJ Open. 2015 Mar 17;5(3):e005966. doi: 10.1136/bmjopen-2014-005966.
The objective of our investigation was to estimate the perinatal mortality rate among institutional births and to compare the sensitivities of different data collection methods.
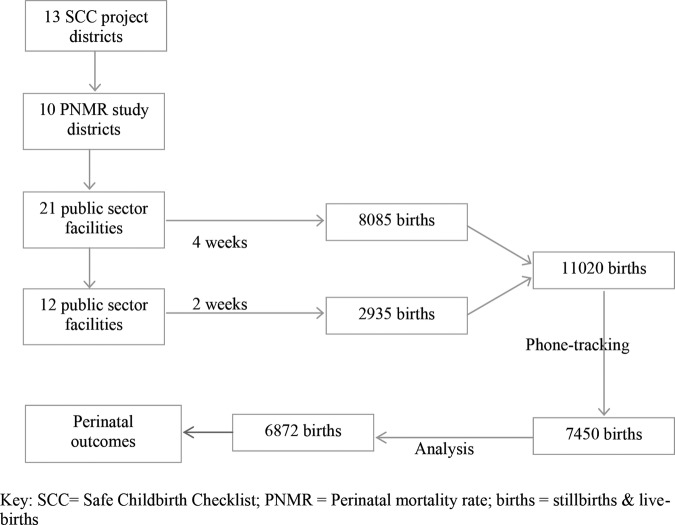
A hospital-based prospective cohort study was undertaken during late-2012 in 21 public sector health facilities of 10 districts of the northern state of Rajasthan, India.
A total of 6872 births were included in this epidemiological study.
Perinatal mortality rate of institutional births was the primary outcome. Sensitivities of 'active' and passive' data collection methods were the secondary outcome measures.
All stillbirth data were from routine government records ('passive system'); early neonatal outcome data from government records ('passive') were compared against the method of 'phone-tracking' of outcomes through the community health worker ('active system'). The Lincoln-Petersen formula for capture-recapture method was used to calculate the probable missing number of early neonatal deaths and thereby estimate the institutional perinatal mortality rate.
Ratio of births in district:subdistrict facilities was 55:45. The estimated perinatal mortality rate (95% CI) by capture-recapture method was 35.8 (34 to 37) per 1000 births. The sensitivity of the passive system was 87-89% while the sensitivity of the active system was 91%. Three-fourths of perinatal deaths were documented as stillbirths. However, for these reported intrauterine deaths or stillbirths, clinical classification by typologies (term vs preterm; intrapartum vs antepartum; macerated vs fresh; with or without congenital anomalies) was absent in the recording system.
Capture-recapture technique can be used to estimate the institutional perinatal mortality rate and also to assess the level of under-reporting by the 'passive' government reporting system. This can subsequently be used for monitoring of trends and studying the impact of health interventions. Accurate clinical categorisation of perinatal deaths is also recommended for improving quality of care.
我们调查的目的是估计机构分娩中的围产期死亡率,并比较不同数据收集方法的敏感性。
2012年末在印度拉贾斯坦邦北部10个区的21家公共部门卫生机构进行了一项基于医院的前瞻性队列研究。
本流行病学研究共纳入6872例分娩。
机构分娩的围产期死亡率是主要结局。“主动”和“被动”数据收集方法的敏感性是次要结局指标。
所有死产数据来自常规政府记录(“被动系统”);将政府记录(“被动”)中的早期新生儿结局数据与通过社区卫生工作者进行结局“电话追踪”的方法(“主动系统”)进行比较。采用捕获-再捕获法的林肯-彼得森公式计算早期新生儿死亡可能遗漏的数量,从而估计机构围产期死亡率。
地区与分区设施的分娩比例为55:45。采用捕获-再捕获法估计的围产期死亡率(95%CI)为每1000例分娩35.8(34至37)例。被动系统的敏感性为87-89%,而主动系统的敏感性为91%。四分之三的围产期死亡被记录为死产。然而,对于这些报告的宫内死亡或死产,记录系统中缺乏按类型(足月与早产;产时与产前;浸软与新鲜;有无先天性异常)进行的临床分类。
捕获-再捕获技术可用于估计机构围产期死亡率,并评估“被动”政府报告系统的漏报水平。随后可用于监测趋势和研究卫生干预措施的影响。还建议对围产期死亡进行准确的临床分类,以提高护理质量。