Ospina-Tascón Gustavo A, Umaña Mauricio, Bermúdez William, Bautista-Rincón Diego F, Hernandez Glenn, Bruhn Alejandro, Granados Marcela, Salazar Blanca, Arango-Dávila César, De Backer Daniel
Intensive Care Unit, Fundación Valle Del Lili - Universidad ICESI, Av. Simón Bolívar Cra. 98, Cali, Colombia,
Intensive Care Med. 2015 May;41(5):796-805. doi: 10.1007/s00134-015-3720-6. Epub 2015 Mar 20.
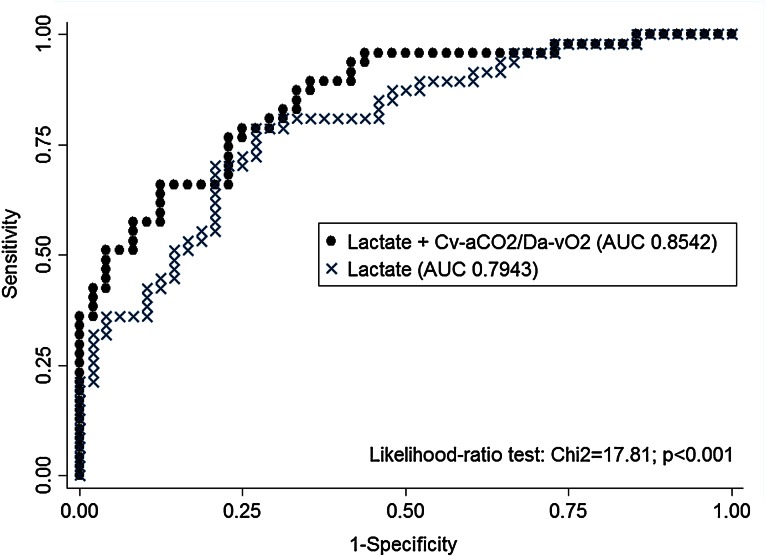
To evaluate the prognostic value of the Cv-aCO2/Da-vO2 ratio combined with lactate levels during the early phases of resuscitation in septic shock.
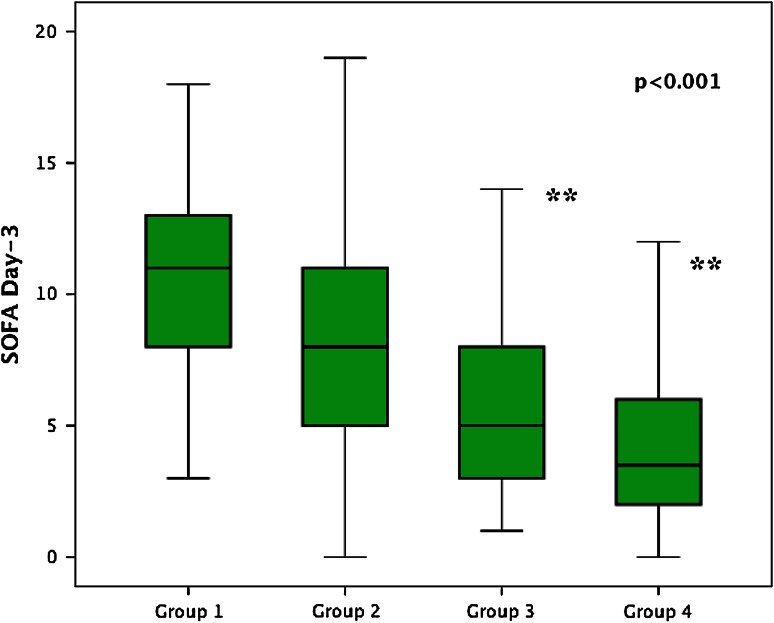
Prospective observational study in a 60-bed mixed ICU. One hundred and thirty-five patients with septic shock were included. The resuscitation protocol targeted mean arterial pressure, pulse pressure variations or central venous pressure, mixed venous oxygen saturation, and lactate levels. Patients were classified into four groups according to lactate levels and Cv-aCO2/Da-vO2 ratio at 6 h of resuscitation (T6): group 1, lactate ≥2.0 mmol/L and Cv-aCO2/Da-vO2 >1.0; group 2, lactate ≥2.0 mmol/L and Cv-aCO2/Da-vO2 ≤1.0; group 3, lactate <2.0 mmol/L and Cv-aCO2/Da-vO2 >1.0; and group 4, lactate <2.0 mmol/L and Cv-aCO2/Da-vO2 ≤1.0.
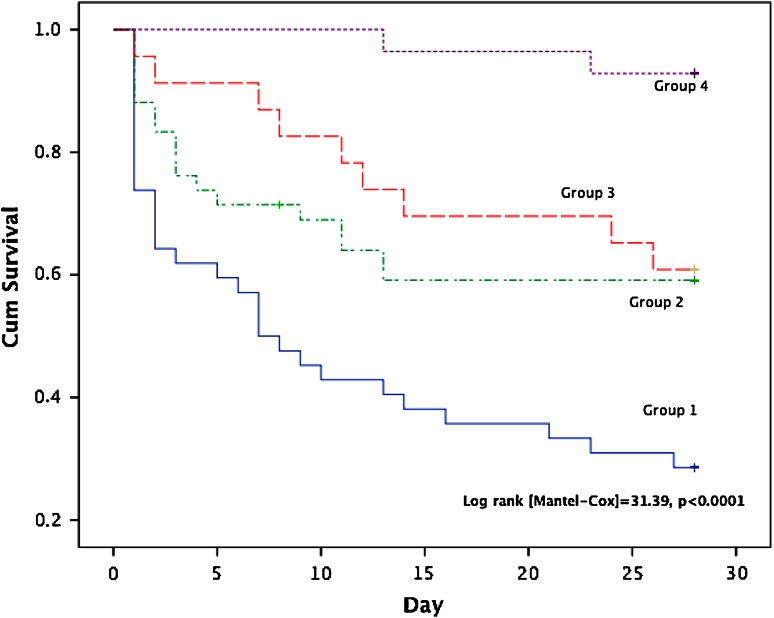
Combination of hyperlactatemia and high Cv-aCO2/Da-vO2 ratio was associated with the worst SOFA scores and lower survival rates at day 28 [log rank (Mantel-Cox) = 31.39, p < 0.0001]. Normalization of both variables was associated with the best outcomes. Patients with a high Cv-aCO2/Da-vO2 ratio and lactate <2.0 mmol/L had similar outcomes to hyperlactatemic patients with low Cv-aCO2/Da-vO2 ratio. The multivariate analysis revealed that Cv-aCO2/Da-vO2 ratio at both T0 (RR 3.85; 95 % CI 1.60-9.27) and T6 (RR 3.97; 95 % CI 1.54-10.24) was an independent predictor for mortality at day 28, as well as lactate levels at T6 (RR 1.58; 95 % CI 1.13-2.22).
Complementing lactate assessment with Cv-aCO2/Da-vO2 ratio during early stages of resuscitation of septic shock can better identify patients at high risk of adverse outcomes. The Cv-aCO2/Da-vO2 ratio may become a potential resuscitation goal in patients with septic shock.
评估脓毒性休克复苏早期中心静脉-动脉血二氧化碳分压差与动脉-静脉血氧含量差(Cv-aCO2/Da-vO2)比值联合乳酸水平的预后价值。
在一家拥有60张床位的综合性重症监护病房(ICU)进行前瞻性观察研究。纳入135例脓毒性休克患者。复苏方案以平均动脉压、脉压变异或中心静脉压、混合静脉血氧饱和度和乳酸水平为目标。根据复苏6小时(T6)时的乳酸水平和Cv-aCO2/Da-vO2比值将患者分为四组:第1组,乳酸≥2.0 mmol/L且Cv-aCO2/Da-vO2>1.0;第2组,乳酸≥2.0 mmol/L且Cv-aCO2/Da-vO2≤1.0;第3组,乳酸<2.0 mmol/L且Cv-aCO2/Da-vO2>1.0;第4组,乳酸<2.0 mmol/L且Cv-aCO2/Da-vO2≤1.0。
高乳酸血症与高Cv-aCO2/Da-vO2比值相结合与第28天最差的序贯器官衰竭评估(SOFA)评分和较低的生存率相关[对数秩检验(Mantel-Cox)=31.39,p<0.0001]。两个变量的正常化与最佳预后相关。Cv-aCO2/Da-vO2比值高且乳酸<2.0 mmol/L的患者与Cv-aCO2/Da-vO2比值低的高乳酸血症患者预后相似。多因素分析显示,T0时(风险比[RR] 3.85;95%置信区间[CI] 1.60-9.27)和T6时的Cv-aCO2/Da-vO2比值(RR 3.97;95% CI 1.54-10.24)以及T6时的乳酸水平(RR 1.58;95% CI 1.13-2.22)是第28天死亡率的独立预测因素。
在脓毒性休克复苏早期,用Cv-aCO2/Da-vO2比值补充乳酸评估可以更好地识别不良结局高危患者。Cv-aCO2/Da-vO2比值可能成为脓毒性休克患者潜在的复苏目标。