Talaat Kawsar R, Babu Subash, Menon Pradeep, Kumarasamy N, Sharma Jabin, Arumugam Jeeva, Dhakshinamurthy Kalaivani, Srinivasan Ramalingam, Poongulali S, Gu Wenjuan, Fay Michael P, Swaminathan Soumya, Nutman Thomas B
Laboratory of Parasitic Diseases, National Institute of Allergy and Infectious Disease, National Institutes of Health, Bethesda, Maryland, United States of America; Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
PLoS Negl Trop Dis. 2015 Mar 20;9(3):e0003622. doi: 10.1371/journal.pntd.0003622. eCollection 2015 Mar.
The disease course of human immunodeficiency virus (HIV) is often altered by existing or newly acquired coincident infections.
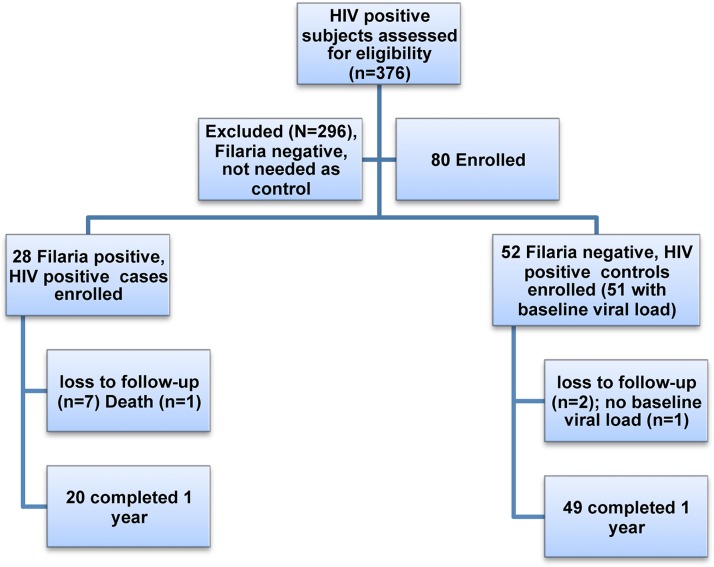
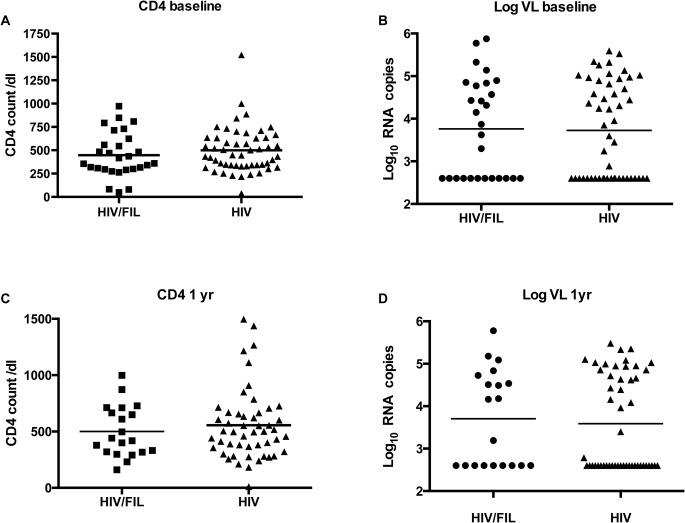
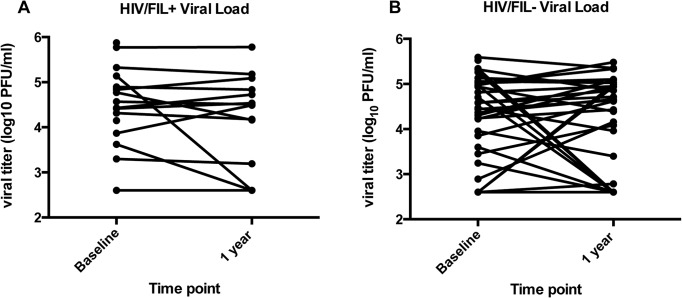
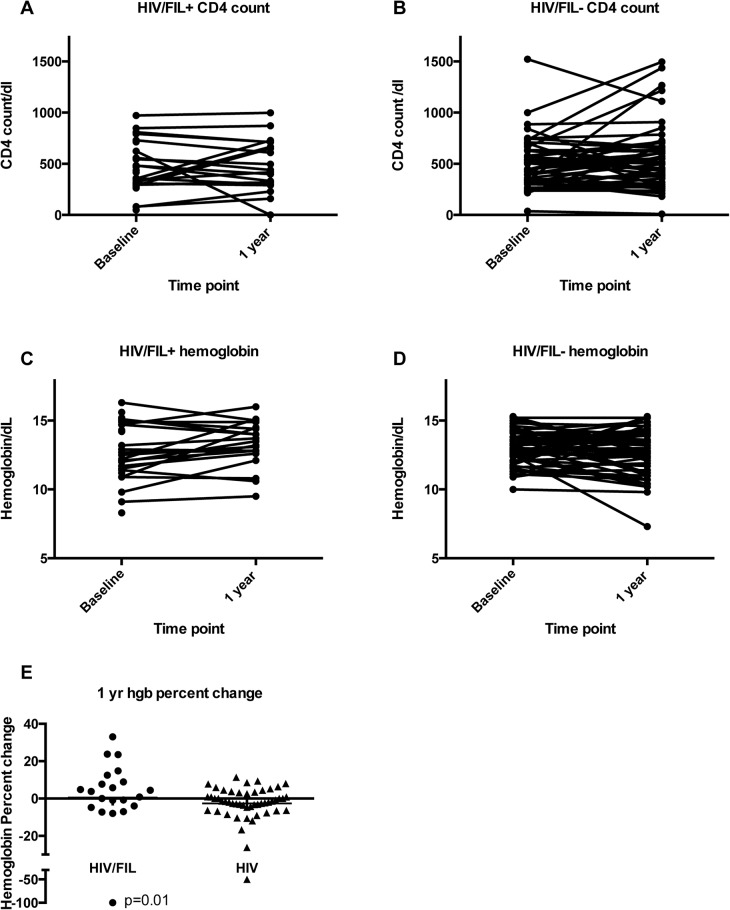
METHODOLOGY/PRINCIPAL FINDINGS: To assess the influence of pre-existing Wuchereria bancrofti infection on HIV progression, we performed a case-controlled treatment study of HIV positive individuals with (FIL+) or without (FIL-) W. bancrofti infection. Twenty-eight HIV+/FIL+ and 51 matched HIV+/FIL- subjects were treated with a single dose of diethylcarbamazine and albendazole (DEC/Alb) and followed for a year at regular intervals. Sixteen of the HIV+/FIL+ subjects (54%) and 28 of the HIV+/FIL- controls (57%) were on antiretroviral therapy (ART) during the study. Following treatment, no differences were noted in clinical outcomes between the 2 groups. There also was no significant difference between the groups in the HIV viral load at 12 months as a percentage of baseline viral load (HIV+/FIL+ group had on average 0.97 times the response of the HIV+/FIL- group, 95% CI 0.88, 1.07) between the groups. Furthermore, there were no significant differences found in either the change in viral load at 1, 3, or 6 months or in the change in CD4 count at 3, 6, or 12 months between the 2 groups.
CONCLUSIONS/SIGNIFICANCE: We were unable to find a significant effect of W. bancrofti infection or its treatment on HIV clinical course or surrogate markers of HIV disease progression though we recognized that our study was limited by the smaller than predicted sample size and by the use of ART in half of the patients. Treatment of W. bancrofti coinfection in HIV positive subjects (as is usual in mass drug administration campaigns) did not represent an increased risk to the subjects, and should therefore be considered for PLWHA living in W. bancrofti endemic areas.
ClinicalTrials.gov NCT00344279.
人类免疫缺陷病毒(HIV)的病程常因现有的或新感染的合并感染而改变。
方法/主要发现:为评估既往感染班氏吴策线虫对HIV病情进展的影响,我们对感染(FIL+)或未感染(FIL-)班氏吴策线虫的HIV阳性个体进行了一项病例对照治疗研究。28例HIV+/FIL+和51例匹配的HIV+/FIL-受试者接受了单剂量的乙胺嗪和阿苯达唑(DEC/Alb)治疗,并定期随访一年。研究期间,16例HIV+/FIL+受试者(54%)和28例HIV+/FIL-对照受试者(57%)接受了抗逆转录病毒治疗(ART)。治疗后,两组的临床结局无差异。两组在12个月时的HIV病毒载量相对于基线病毒载量的百分比也无显著差异(HIV+/FIL+组的反应平均是HIV+/FIL-组的0.97倍,95%可信区间为0.88, 1.07)。此外,两组在1、3或6个月时的病毒载量变化以及在3、6或12个月时的CD4细胞计数变化均无显著差异。
结论/意义:尽管我们认识到本研究受样本量小于预期以及一半患者使用ART的限制,但我们未能发现班氏吴策线虫感染或其治疗对HIV临床病程或HIV疾病进展替代指标有显著影响。在HIV阳性受试者中治疗班氏吴策线虫合并感染(大规模药物给药运动中常见)对受试者并不意味着风险增加,因此对于生活在班氏吴策线虫流行地区的艾滋病毒感染者应考虑进行治疗。
ClinicalTrials.gov NCT00344279。