Rickards Caroline A, Sprick Justin D, Colby Hannah B, Kay Victoria L, Tzeng Yu-Chieh
Department of Integrative Physiology & Anatomy, University of North Texas Health Science Center, 3500 Camp Bowie Boulevard, Fort Worth, TX 76107, USA.
Physiol Meas. 2015 Apr;36(4):785-801. doi: 10.1088/0967-3334/36/4/785. Epub 2015 Mar 23.
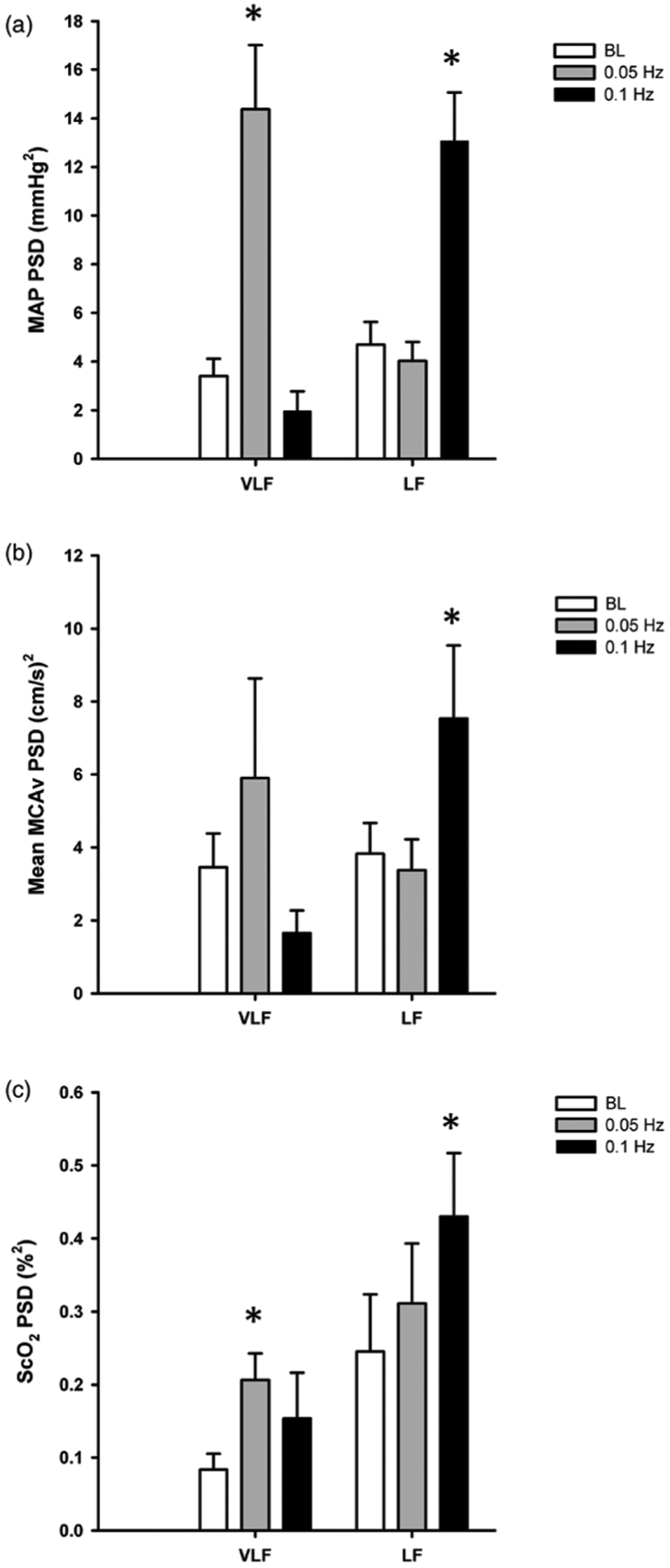
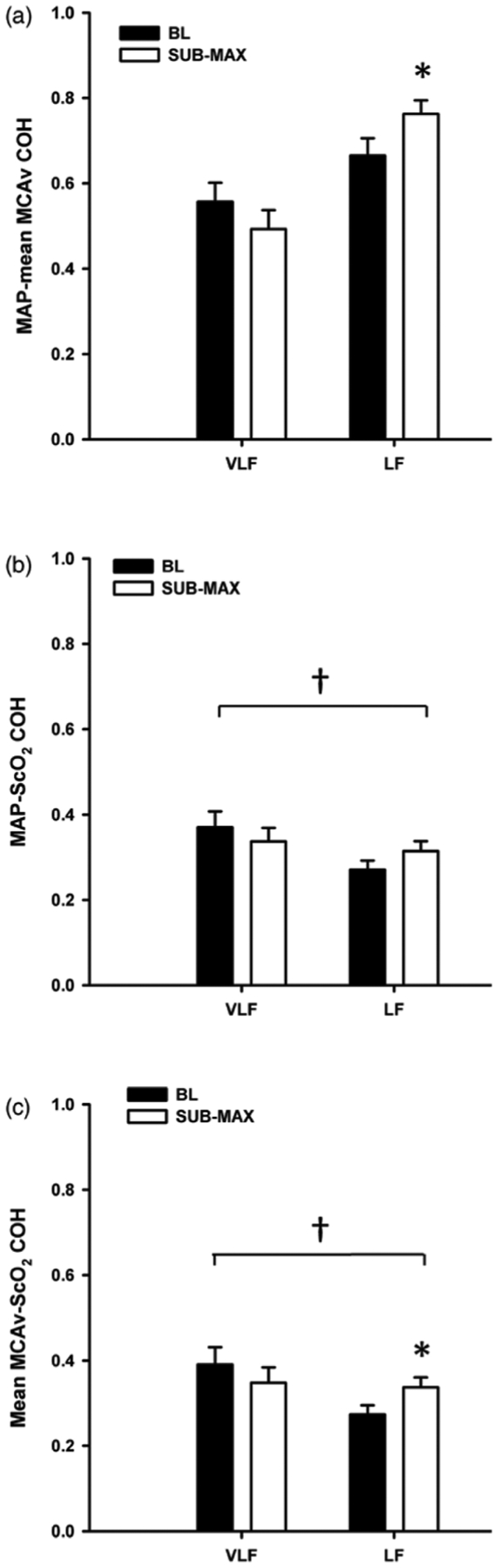
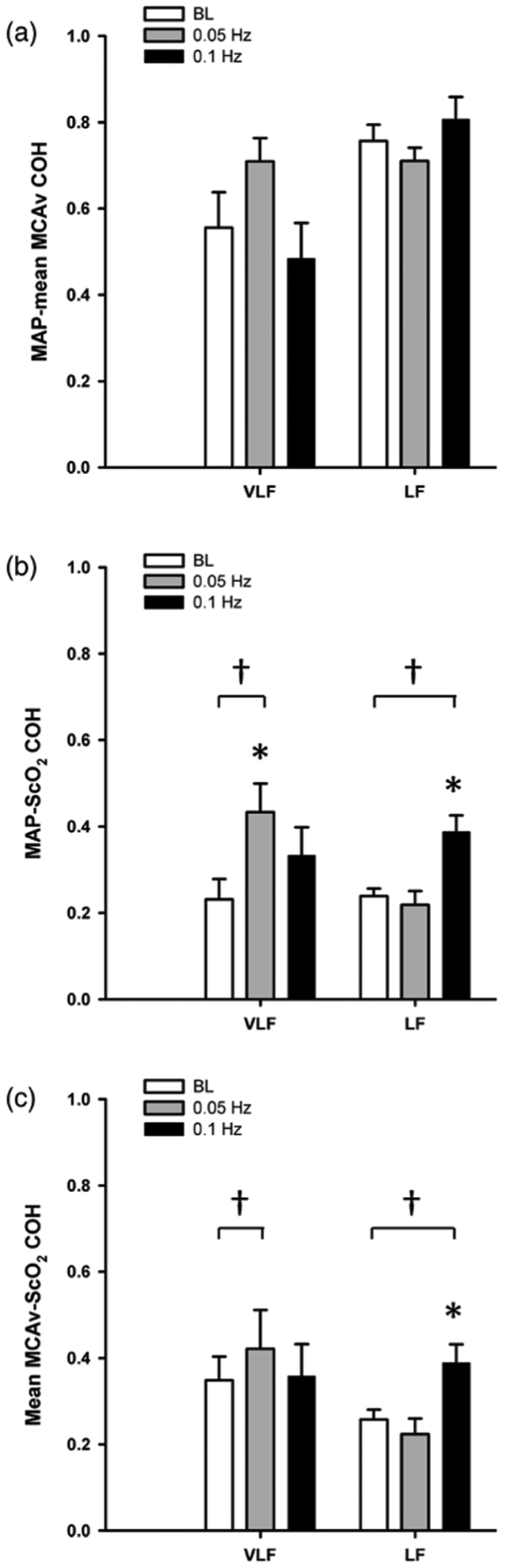
We tested the hypothesis that transmission of arterial pressure to brain tissue oxygenation is low under conditions of arterial pressure instability. Two experimental models of hemodynamic instability were used in healthy human volunteers; (1) oscillatory lower body negative pressure (OLBNP) (N = 8; 5 male, 3 female), and; (2) maximal LBNP to presyncope (N = 21; 13 male, 8 female). Mean arterial pressure (MAP), middle cerebral artery velocity (MCAv), and cerebral tissue oxygen saturation (ScO2) were measured non-invasively. For the OLBNP protocol, between 0 and -60 mmHg negative pressure was applied for 20 cycles at 0.05 Hz, then 20 cycles at 0.1 Hz. For the maximal LBNP protocol, progressive 5 min stages of chamber decompression were applied until the onset of presyncope. Spectral power of MAP, mean MCAv, and ScO2 were calculated within the VLF (0.04-0.07 Hz), and LF (0.07-0.2 Hz) ranges, and cross-spectral coherence was calculated for MAP-mean MCAv, MAP-ScO2, and mean MCAv-ScO2 at baseline, during each OLBNP protocol, and at the level prior to pre-syncope during maximal LBNP (sub-max). The key findings are (1) both 0.1 Hz OLBNP and sub-max LBNP elicited increases in LF power for MAP, mean MCAv, and ScO2 (p ≤ 0.08); (2) 0.05 Hz OLBNP increased VLF power in MAP and ScO2 only (p ≤ 0.06); (3) coherence between MAP-mean MCAv was consistently higher (≥0.71) compared with MAP-ScO2, and mean MCAv-ScO2 (≤0.43) during both OLBNP protocols, and sub-max LBNP (p ≤ 0.04). These data indicate high linearity between pressure and cerebral blood flow variations, but reduced linearity between cerebral tissue oxygenation and both arterial pressure and cerebral blood flow. Measuring arterial pressure variability may not always provide adequate information about the downstream effects on cerebral tissue oxygenation, the key end-point of interest for neuronal viability.
在动脉压不稳定的情况下,动脉压向脑组织氧合的传递较低。在健康人类志愿者中使用了两种血流动力学不稳定的实验模型:(1)振荡性下体负压(OLBNP)(N = 8;5名男性,3名女性),以及;(2)最大下体负压至接近晕厥(N = 21;13名男性,8名女性)。采用非侵入性方法测量平均动脉压(MAP)、大脑中动脉血流速度(MCAv)和脑组织氧饱和度(ScO2)。对于OLBNP方案,在0至-60 mmHg负压下以0.05 Hz施加20个周期,然后以0.1 Hz施加20个周期。对于最大下体负压方案,逐步进行5分钟的舱室减压阶段,直到接近晕厥发作。在甚低频(0.04 - 0.07 Hz)和低频(0.07 - 0.2 Hz)范围内计算MAP、平均MCAv和ScO2的频谱功率,并在基线、每个OLBNP方案期间以及最大下体负压接近晕厥前水平(次最大)计算MAP - 平均MCAv、MAP - ScO2和平均MCAv - ScO2之间的交叉谱相干性。主要发现为:(1)0.1 Hz的OLBNP和次最大下体负压均引起MAP、平均MCAv和ScO2的低频功率增加(p≤0.08);(2)0.05 Hz的OLBNP仅增加MAP和ScO2中的甚低频功率(p≤0.06);(3)在两个OLBNP方案和次最大下体负压期间,MAP - 平均MCAv之间的相干性始终高于MAP - ScO2和平均MCAv - ScO2(p≤0.04)。这些数据表明压力与脑血流变化之间具有高度线性,但脑组织氧合与动脉压和脑血流之间的线性降低。测量动脉压变异性可能并不总是能提供关于对脑组织氧合下游影响的充分信息,而脑组织氧合是神经元存活能力的关键关注终点。