Lancet Neurol. 2015 May;14(5):485-96. doi: 10.1016/S1474-4422(15)00012-5. Epub 2015 Mar 27.
Brain scans are essential to exclude haemorrhage in patients with suspected acute ischaemic stroke before treatment with alteplase. However, patients with early ischaemic signs could be at increased risk of haemorrhage after alteplase treatment, and little information is available about whether pre-existing structural signs, which are common in older patients, affect response to alteplase. We aimed to investigate the association between imaging signs on brain CT and outcomes after alteplase.
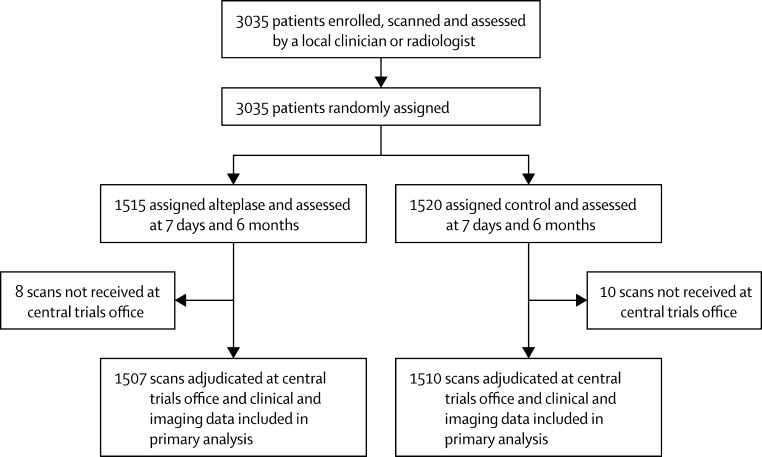
IST-3 was a multicentre, randomised controlled trial of intravenous alteplase (0·9 mg/kg) versus control within 6 h of acute ischaemic stroke. The primary outcome was independence at 6 months (defined as an Oxford Handicap Scale [OHS] score of 0-2). 3035 patients were enrolled to IST-3 and underwent prerandomisation brain CT. Experts who were unaware of the random allocation assessed scans for early signs of ischaemia (tissue hypoattenuation, infarct extent, swelling, and hyperattenuated artery) and pre-existing signs (old infarct, leukoaraiosis, and atrophy). In this prespecified analysis, we assessed interactions between these imaging signs, symptomatic intracranial haemorrhage (a secondary outcome in IST-3) and independence at 6 months, and alteplase, adjusting for age, National Institutes of Health Stroke Scale (NIHSS) score, and time to randomisation. This trial is registered at ISRCTN.com, number ISRCTN25765518.
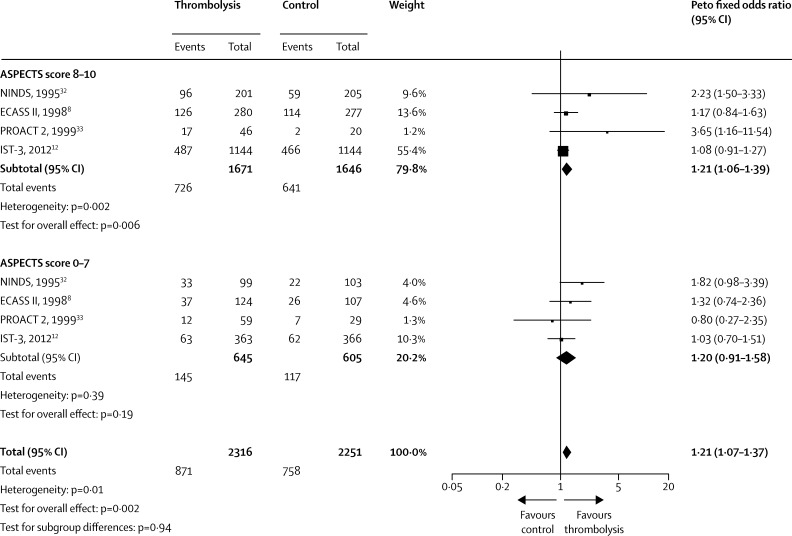
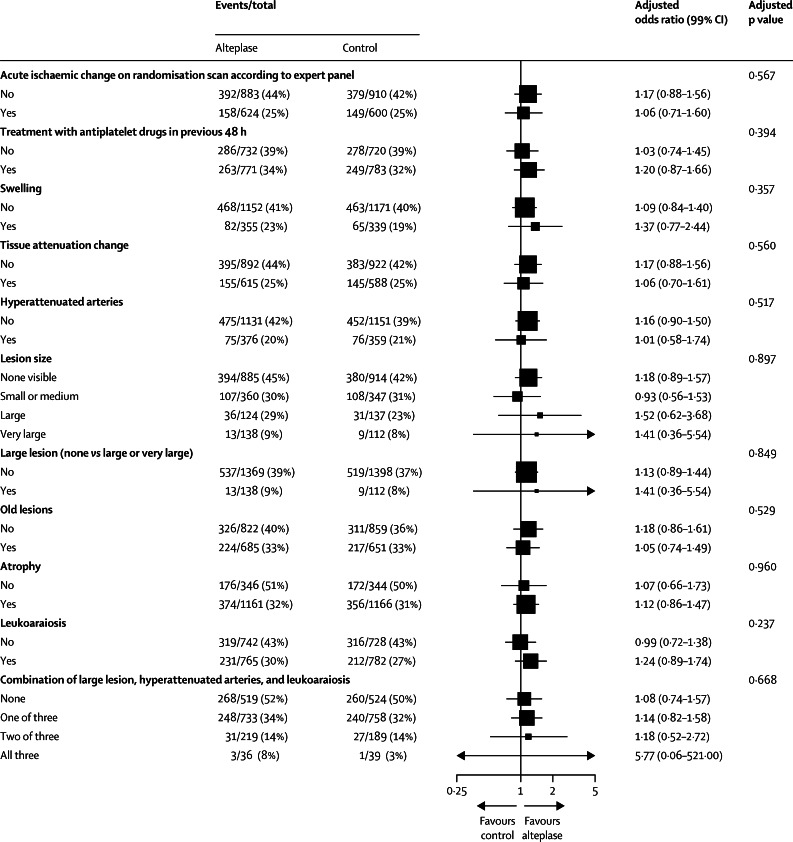
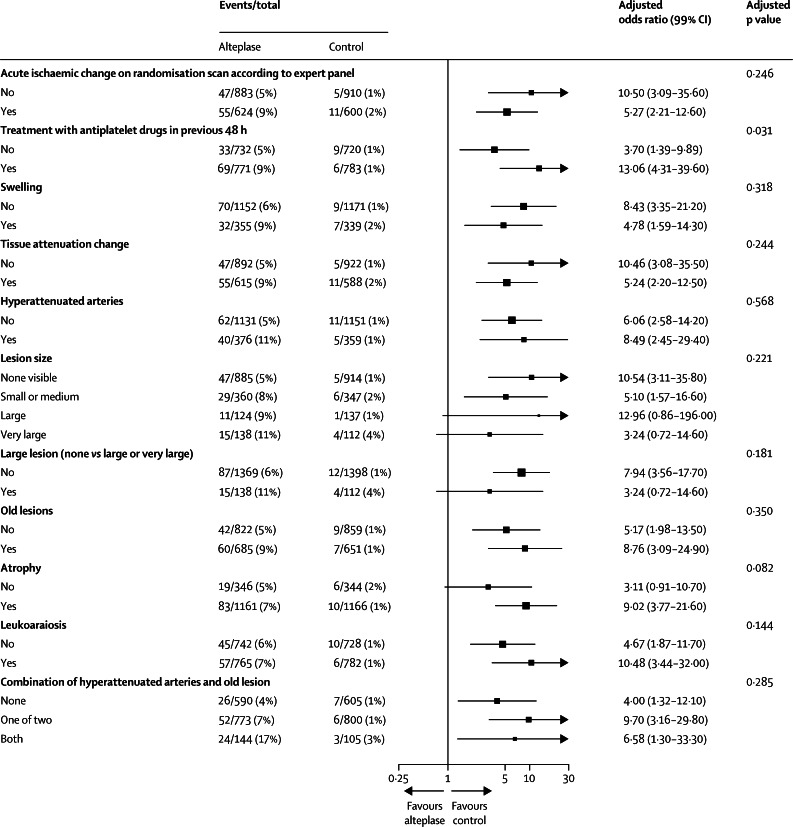
3017 patients were assessed in this analysis, of whom 1507 were allocated alteplase and 1510 were assigned control. A reduction in independence was predicted by tissue hypoattenuation (odds ratio 0·66, 95% CI 0·55-0·81), large lesion (0·51, 0·38-0·68), swelling (0·59, 0·46-0·75), hyperattenuated artery (0·59, 0·47-0·75), atrophy (0·74, 0·59-0·94), and leukoaraiosis (0·72, 0·59-0·87). Symptomatic intracranial haemorrhage was predicted by old infarct (odds ratio 1·72, 95% CI 1·18-2·51), tissue hypoattenuation (1·54, 1·04-2·27), and hyperattenuated artery (1·54, 1·03-2·29). Some combinations of signs increased the absolute risk of symptomatic intracranial haemorrhage (eg, both old infarct and hyperattenuated artery, excess with alteplase 13·8%, 95% CI 6·9-20·7; both signs absent, excess 3·2%, 1·4-5·1). However, no imaging findings-individually or combined-modified the effect of alteplase on independence or symptomatic intracranial haemorrhage.
Some early ischaemic and pre-existing signs were associated with reduced independence at 6 months and increased symptomatic intracranial haemorrhage. Although no interaction was noted between brain imaging signs and effects of alteplase on these outcomes, some combinations of signs increased some absolute risks. Pre-existing signs should be considered, in addition to early ischaemic signs, during the assessment of patients with acute ischaemic stroke.
UK Medical Research Council, Health Foundation UK, Stroke Association UK, Chest Heart Stroke Scotland, Scottish Funding Council SINAPSE Collaboration, and multiple governmental and philanthropic national funders.
在使用阿替普酶治疗疑似急性缺血性卒中患者前,脑部扫描对于排除出血至关重要。然而,有早期缺血征象的患者在接受阿替普酶治疗后发生出血的风险可能增加,而且关于老年患者中常见的既往结构性征象是否会影响对阿替普酶的反应,目前几乎没有相关信息。我们旨在研究脑部CT成像征象与阿替普酶治疗后的结局之间的关联。
IST-3是一项多中心随机对照试验,在急性缺血性卒中6小时内,比较静脉注射阿替普酶(0.9mg/kg)与对照组。主要结局是6个月时的独立状态(定义为牛津残疾量表[OHS]评分为0-2)。3035例患者纳入IST-3并在随机分组前接受脑部CT检查。对随机分组不知情的专家评估扫描结果,以确定缺血早期征象(组织低密度、梗死范围、肿胀和动脉高密度)和既往征象(陈旧性梗死、脑白质疏松和萎缩)。在这项预先设定的分析中,我们评估了这些成像征象、症状性颅内出血(IST-3的次要结局)和6个月时的独立状态之间的相互作用,以及阿替普酶的作用,并对年龄、美国国立卫生研究院卒中量表(NIHSS)评分和随机分组时间进行了校正。该试验在ISRCTN.com注册,注册号为ISRCTN25765518。
本分析评估了3017例患者,其中1507例分配接受阿替普酶治疗,1510例分配接受对照组治疗。组织低密度(比值比0.66,95%CI 0.55-0.81)、大病灶(0.51,0.38-0.68)、肿胀(0.59,0.46-0.75)、动脉高密度(0.59,0.47-0.75)、萎缩(0.74,0.59-0.94)和脑白质疏松(0.72,0.59-0.87)提示6个月时独立状态降低。陈旧性梗死(比值比1.72,95%CI 1.18-2.51)、组织低密度(1.54,1.04-2.27)和动脉高密度(1.54,1.03-2.29)提示症状性颅内出血。某些征象组合增加了症状性颅内出血的绝对风险(例如,既有陈旧性梗死又有动脉高密度,阿替普酶治疗组额外风险为13.8%,95%CI 6.9-20.7;两者均无,额外风险为3.2%,1.4-5.1)。然而,没有影像学发现——单独或联合——改变阿替普酶对独立状态或症状性颅内出血的影响。
一些早期缺血和既往征象与6个月时独立状态降低及症状性颅内出血增加有关。虽然未发现脑成像征象与阿替普酶对这些结局的影响之间存在相互作用,但某些征象组合增加了一些绝对风险。在评估急性缺血性卒中患者时,除了早期缺血征象外,还应考虑既往征象。
英国医学研究理事会、英国健康基金会、英国卒中协会、苏格兰胸部心脏卒中协会、苏格兰资助委员会SINAPSE合作项目以及多个政府和慈善性质的国家资助机构。