Mocroft Amanda, Lundgren Jens D, Ross Michael, Law Matthew, Reiss Peter, Kirk Ole, Smith Colette, Wentworth Deborah, Neuhaus Jacqueline, Fux Christoph A, Moranne Olivier, Morlat Phillipe, Johnson Margaret A, Ryom Lene
Department of Infection and Population Health, University College London, London, United Kingdom.
Copenhagen HIV Programme, Department of Infectious Diseases, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
PLoS Med. 2015 Mar 31;12(3):e1001809. doi: 10.1371/journal.pmed.1001809. eCollection 2015 Mar.
Chronic kidney disease (CKD) is a major health issue for HIV-positive individuals, associated with increased morbidity and mortality. Development and implementation of a risk score model for CKD would allow comparison of the risks and benefits of adding potentially nephrotoxic antiretrovirals to a treatment regimen and would identify those at greatest risk of CKD. The aims of this study were to develop a simple, externally validated, and widely applicable long-term risk score model for CKD in HIV-positive individuals that can guide decision making in clinical practice.
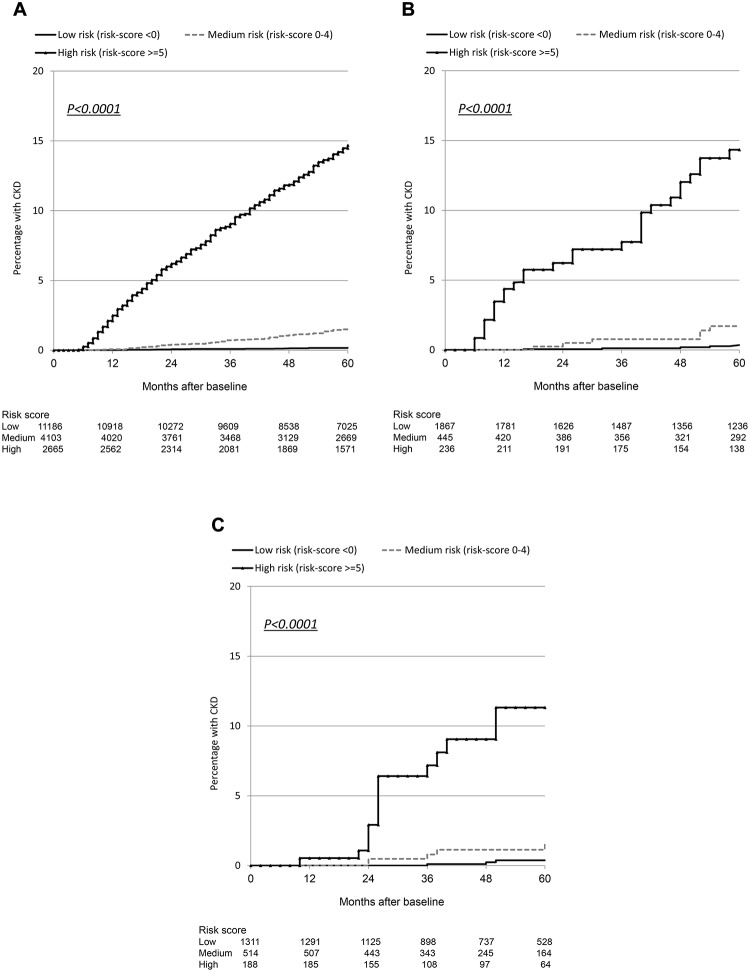
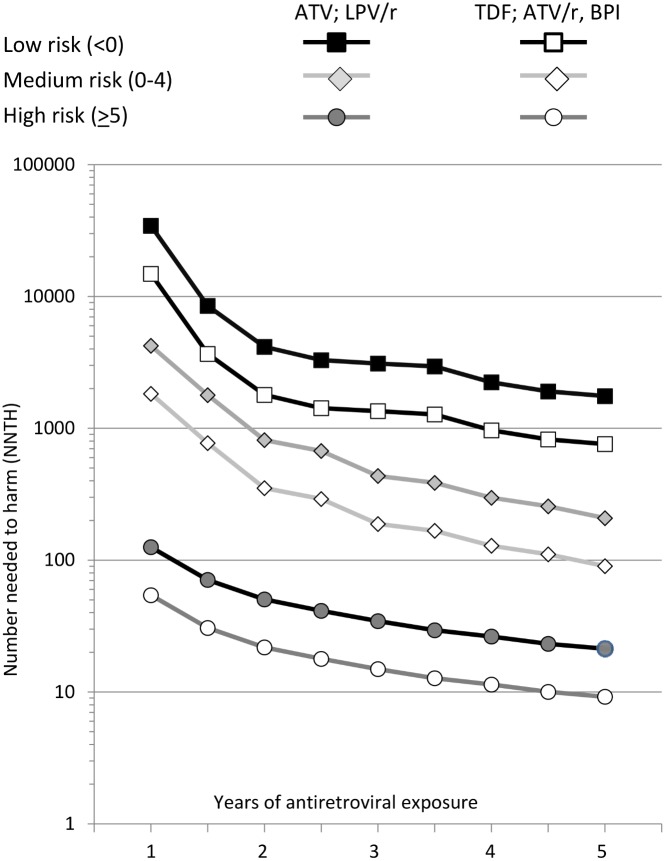
A total of 17,954 HIV-positive individuals from the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) study with ≥3 estimated glomerular filtration rate (eGFR) values after 1 January 2004 were included. Baseline was defined as the first eGFR > 60 ml/min/1.73 m2 after 1 January 2004; individuals with exposure to tenofovir, atazanavir, atazanavir/ritonavir, lopinavir/ritonavir, other boosted protease inhibitors before baseline were excluded. CKD was defined as confirmed (>3 mo apart) eGFR ≤ 60 ml/min/1.73 m2. Poisson regression was used to develop a risk score, externally validated on two independent cohorts. In the D:A:D study, 641 individuals developed CKD during 103,185 person-years of follow-up (PYFU; incidence 6.2/1,000 PYFU, 95% CI 5.7-6.7; median follow-up 6.1 y, range 0.3-9.1 y). Older age, intravenous drug use, hepatitis C coinfection, lower baseline eGFR, female gender, lower CD4 count nadir, hypertension, diabetes, and cardiovascular disease (CVD) predicted CKD. The adjusted incidence rate ratios of these nine categorical variables were scaled and summed to create the risk score. The median risk score at baseline was -2 (interquartile range -4 to 2). There was a 1:393 chance of developing CKD in the next 5 y in the low risk group (risk score < 0, 33 events), rising to 1:47 and 1:6 in the medium (risk score 0-4, 103 events) and high risk groups (risk score ≥ 5, 505 events), respectively. Number needed to harm (NNTH) at 5 y when starting unboosted atazanavir or lopinavir/ritonavir among those with a low risk score was 1,702 (95% CI 1,166-3,367); NNTH was 202 (95% CI 159-278) and 21 (95% CI 19-23), respectively, for those with a medium and high risk score. NNTH was 739 (95% CI 506-1462), 88 (95% CI 69-121), and 9 (95% CI 8-10) for those with a low, medium, and high risk score, respectively, starting tenofovir, atazanavir/ritonavir, or another boosted protease inhibitor. The Royal Free Hospital Clinic Cohort included 2,548 individuals, of whom 94 individuals developed CKD (3.7%) during 18,376 PYFU (median follow-up 7.4 y, range 0.3-12.7 y). Of 2,013 individuals included from the SMART/ESPRIT control arms, 32 individuals developed CKD (1.6%) during 8,452 PYFU (median follow-up 4.1 y, range 0.6-8.1 y). External validation showed that the risk score predicted well in these cohorts. Limitations of this study included limited data on race and no information on proteinuria.
Both traditional and HIV-related risk factors were predictive of CKD. These factors were used to develop a risk score for CKD in HIV infection, externally validated, that has direct clinical relevance for patients and clinicians to weigh the benefits of certain antiretrovirals against the risk of CKD and to identify those at greatest risk of CKD.
慢性肾脏病(CKD)是HIV阳性个体面临的一个主要健康问题,与发病率和死亡率增加相关。开发并实施CKD风险评分模型将有助于比较在治疗方案中添加潜在肾毒性抗逆转录病毒药物的风险和益处,并能识别出CKD风险最高的个体。本研究的目的是为HIV阳性个体开发一种简单、经过外部验证且广泛适用的CKD长期风险评分模型,以指导临床实践中的决策。
纳入了抗HIV药物不良事件数据收集(D:A:D)研究中自2004年1月1日后有≥3个估计肾小球滤过率(eGFR)值的17954例HIV阳性个体。基线定义为2004年1月1日后首个eGFR>60 ml/min/1.73 m²;排除在基线前暴露于替诺福韦、阿扎那韦、阿扎那韦/利托那韦、洛匹那韦/利托那韦或其他增效蛋白酶抑制剂的个体。CKD定义为确诊的(间隔>3个月)eGFR≤60 ml/min/1.73 m²。采用泊松回归开发风险评分,并在两个独立队列中进行外部验证。在D:A:D研究中,641例个体在103185人年的随访(PYFU)期间发生CKD(发病率6.2/1000 PYFU,95%CI 5.7 - 6.7;中位随访6.1年,范围0.3 - 9.1年)。年龄较大、静脉吸毒、丙型肝炎合并感染、基线eGFR较低、女性、CD4细胞计数最低点较低、高血压、糖尿病和心血管疾病(CVD)可预测CKD。对这九个分类变量的调整发病率比值进行缩放并求和以创建风险评分。基线时风险评分的中位数为 - 2(四分位间距 - 4至2)。低风险组(风险评分<0,33例事件)在未来5年发生CKD的概率为1:393,中风险组(风险评分0 - 4,103例事件)升至1:47,高风险组(风险评分≥5,505例事件)升至1:6。低风险评分者开始使用未增效阿扎那韦或洛匹那韦/利托那韦时5年的伤害所需人数(NNTH)为1702(95%CI 1166 - 3367);中风险评分者和高风险评分者的NNTH分别为202(95%CI 159 - 278)和21(95%CI 19 - 23)。低、中、高风险评分者开始使用替诺福韦、阿扎那韦/利托那韦或其他增效蛋白酶抑制剂时的NNTH分别为739(95%CI 506 - 1462)、88(95%CI 69 - 121)和9(95%CI 8 - 10)。皇家自由医院临床队列包括2548例个体,其中94例个体在18376 PYFU期间发生CKD(3.7%)(中位随访7.4年,范围0.3 - 12.7年)。在来自SMART/ESPRIT对照组的2013例个体中,32例个体在8452 PYFU期间发生CKD(1.6%)(中位随访4.1年,范围0.6 - 8.1年)。外部验证表明该风险评分在这些队列中预测效果良好。本研究的局限性包括种族数据有限且无蛋白尿信息。
传统风险因素和与HIV相关的风险因素均能预测CKD。这些因素被用于开发HIV感染中CKD的风险评分,该评分经过外部验证,对患者和临床医生权衡某些抗逆转录病毒药物的益处与CKD风险以及识别CKD风险最高的个体具有直接临床相关性。