Centre for Clinical Research, Epidemiology, Modelling and Evaluation (CREME), Institute for Global Health, University College London, London, UK.
Centre for Clinical Research, Epidemiology, Modelling and Evaluation (CREME), Institute for Global Health, University College London, London, UK; CHIP, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
Kidney Int. 2024 Jul;106(1):136-144. doi: 10.1016/j.kint.2024.04.010. Epub 2024 May 1.
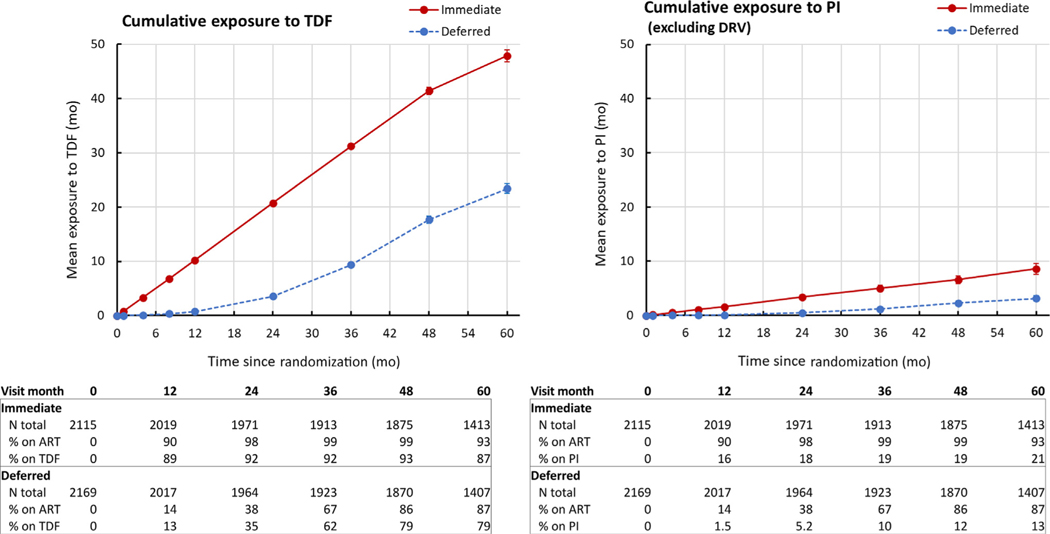
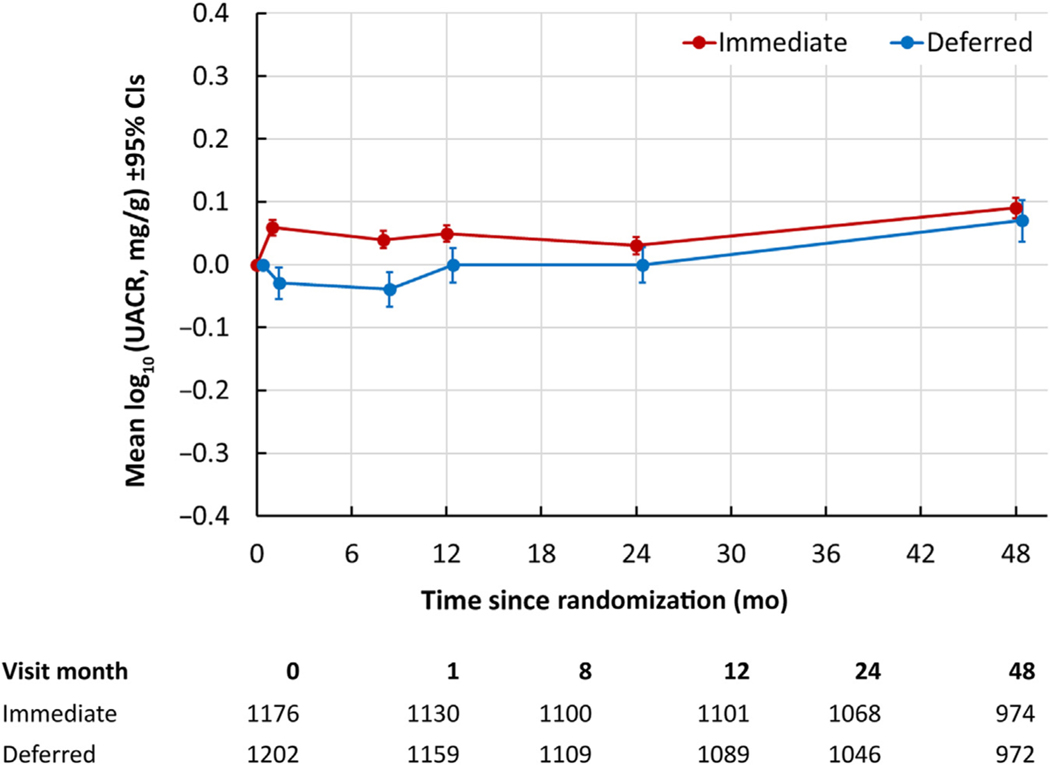
People with human immunodeficiency virus (HIV) are at risk for chronic kidney disease (CKD) due to HIV and antiretroviral therapy (ART) nephrotoxicity. Immediate ART initiation reduces mortality and is now the standard of care, but the long-term impact of prolonged ART exposure on CKD is unknown. To evaluate this, the Strategic Timing of Antiretroviral Treatment (START) trial randomized 4,684 ART-naïve adults with CD4 cell count under 500 cells/mm to immediate versus deferred ART. We previously reported a small but statistically significantly greater decline in estimated glomerular filtration rate (eGFR) over a median of 2.1 years in participants randomized to deferred versus immediate ART. Here, we compare the incidence of CKD events and changes in eGFR and urine albumin/creatinine ratio (UACR) in participants randomized to immediate versus deferred ART during extended follow-up. Over a median of 9.3 years, eight participants experienced kidney failure or kidney-related death, three in the immediate and five in the deferred ART arms, respectively. Over a median of five years of more comprehensive follow-up, the annual rate of eGFR decline was 1.19 mL/min/1.73m/year, with no significant difference between treatment arms (difference deferred - immediate arm 0.055; 95% confidence interval -0.106, 0.217 mL/min/1.73m). Results were similar in models adjusted for baseline covariates associated with CKD, including UACR and APOL1 genotype. Similarly, there was no significant difference between treatment arms in incidence of confirmed UACR 30 mg/g or more (odds ratio 1.13; 95% confidence interval 0.85, 1.51). Thus, our findings provide the most definitive evidence to date in support of the long-term safety of early ART with respect to kidney health.
人类免疫缺陷病毒 (HIV) 感染者由于 HIV 和抗逆转录病毒治疗 (ART) 的肾毒性而面临慢性肾脏病 (CKD) 的风险。立即开始 ART 可降低死亡率,目前已成为标准治疗方法,但长期暴露于 ART 对 CKD 的影响尚不清楚。为了评估这一点,战略时机抗逆转录病毒治疗 (START) 试验将 4684 名 CD4 细胞计数低于 500 个/立方毫米的初次接受 ART 的成年人随机分为立即开始 ART 与延迟开始 ART 两组。我们之前报道过,在中位时间为 2.1 年的随访中,与延迟开始 ART 相比,随机接受立即开始 ART 的参与者估算肾小球滤过率 (eGFR) 下降幅度较小,但具有统计学意义。在此,我们比较了在延长随访期间随机接受立即开始 ART 与延迟开始 ART 的参与者的 CKD 事件发生率以及 eGFR 和尿白蛋白/肌酐比值 (UACR) 的变化。在中位时间为 9.3 年的随访中,8 名参与者发生了肾衰竭或与肾脏相关的死亡,分别有 3 名和 5 名在立即开始 ART 组和延迟开始 ART 组。在中位时间为 5 年的更全面的随访中,eGFR 下降的年率为 1.19 mL/min/1.73m/year,两组之间无显著差异(治疗组之间的差异延迟 - 立即组为 0.055;95%置信区间为 -0.106,0.217 mL/min/1.73m)。在调整了与 CKD 相关的基线协变量(包括 UACR 和 APOL1 基因型)的模型中,结果相似。同样,在治疗组之间,确诊 UACR 为 30 mg/g 或更高的发生率也无显著差异(比值比 1.13;95%置信区间 0.85,1.51)。因此,我们的研究结果提供了迄今为止最明确的证据,支持早期 ART 对肾脏健康的长期安全性。