Choi Ju Young, Jung Sung-Ae, Shim Ki-Nam, Cho Won Young, Keum Bora, Byeon Jeong-Sik, Huh Kyu Chan, Jang Byung Ik, Chang Dong Kyung, Jung Hwoon-Yong, Kong Kyoung Ae
Department of Internal Medicine, Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea.
Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
J Korean Med Sci. 2015 Apr;30(4):398-406. doi: 10.3346/jkms.2015.30.4.398. Epub 2015 Mar 19.
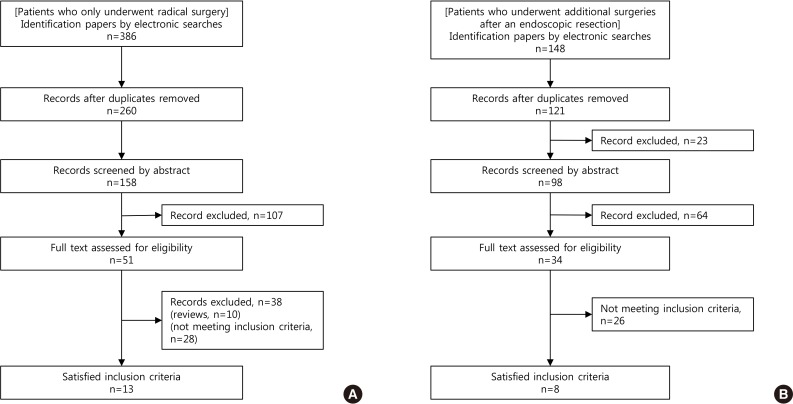
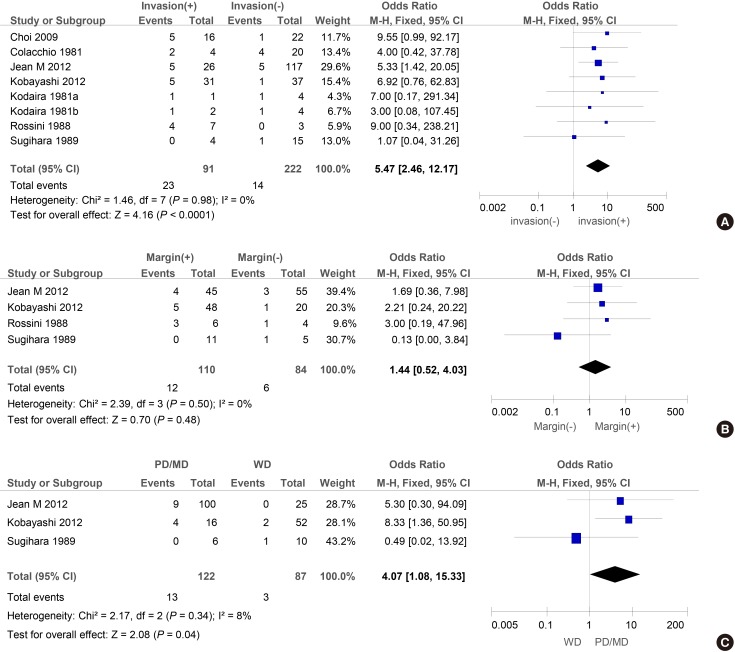
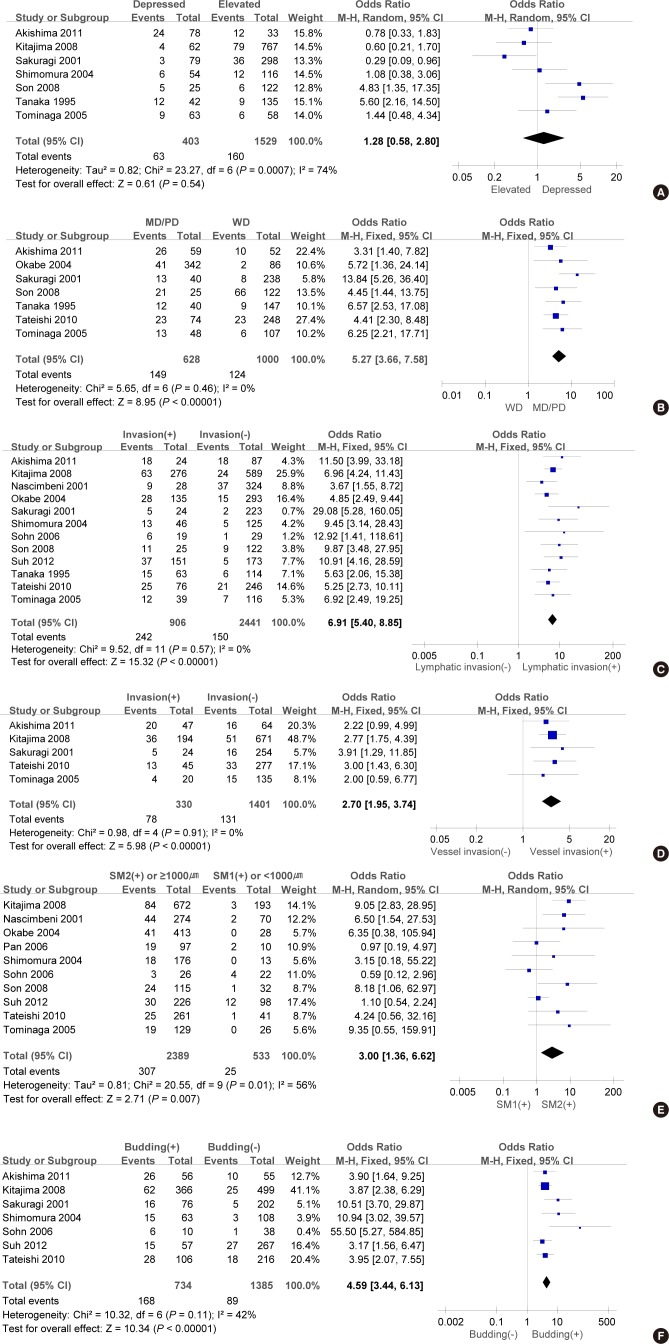
The objective of this study was to conduct a meta-analysis to determine risk factors that may facilitate patient selection for radical resections or additional resections after a polypectomy. Eligible articles were identified by searches of PUBMED, Cochrane Library and Korean Medical Database using the terms (early colorectal carcinoma [ECC], lymph node metastasis [LNM], colectomy, endoscopic resection). Thirteen cohort studies of 7,066 ECC patients who only underwent radical surgery have been analysed. There was a significant risk of LNM when they had submucosal invasion (≥ SM2 or ≥ 1,000 µm) (odds Ratio [OR], 3.00; 95% confidence interval [CI], 1.36-6.62, P = 0.007). Moreover, it has been found that vascular invasion (OR, 2.70; 95% CI, 1.95-3.74; P < 0.001), lymphatic invasion (OR, 6.91; 95% CI, 5.40-8.85; P < 0.001), poorly differentiated carcinomas (OR, 8.27; 95% CI, 4.67-14.66; P < 0.001) and tumor budding (OR, 4.59; 95% CI, 3.44-6.13; P < 0.001) were significantly associated with LNM. Furthermore, another analysis was carried out on eight cohort studies of 310 patients who underwent additional surgeries after an endoscopic resection. The major factors identified in these studies include lymphovascular invasion on polypectomy specimens (OR, 5.47; 95% CI, 2.46-12.17; P < 0.001) and poorly or moderately differentiated carcinomas (OR, 4.07; 95% CI, 1.08-15.33; P = 0.04). For ECC patients with ≥ SM2 or ≥ 1,000 µm submucosal invasion, vascular invasion, lymphatic invasion, poorly differentiated carcinomas or tumor budding, it is deemed that a more extensive resection accompanied by a lymph node dissection is necessary. Even if the lesion is completely removed by an endoscopic resection, an additional surgical resection should be considered in patients with poorly or moderately differentiated carcinomas or lymphovascular invasion.
本研究的目的是进行一项荟萃分析,以确定可能有助于选择接受根治性切除或息肉切除术后追加切除的患者的危险因素。通过使用术语(早期结直肠癌[ECC]、淋巴结转移[LNM]、结肠切除术、内镜切除术)在PUBMED、Cochrane图书馆和韩国医学数据库中进行检索,确定符合条件的文章。对仅接受根治性手术的7066例ECC患者的13项队列研究进行了分析。当他们有黏膜下浸润(≥SM2或≥1000µm)时,发生LNM的风险显著增加(优势比[OR],3.00;95%置信区间[CI],1.36 - 6.62,P = 0.007)。此外,还发现血管浸润(OR,2.70;95%CI,1.95 - 3.74;P < 0.001)、淋巴管浸润(OR,6.91;95%CI,5.40 - 8.85;P < 0.001)、低分化癌(OR,8.27;95%CI,4.67 - 14.66;P < 0.001)和肿瘤芽生(OR,4.59;95%CI,3.44 - 6.13;P < 0.001)与LNM显著相关。此外,对310例在内镜切除术后接受追加手术的患者的8项队列研究进行了另一项分析。这些研究中确定的主要因素包括息肉切除标本中的淋巴管浸润(OR,5.47;95%CI,2.46 - 12.17;P < 0.001)和低分化或中分化癌(OR,4.07;95%CI,1.08 - 15.33;P = 0.04)。对于黏膜下浸润≥SM2或≥1000µm、有血管浸润、淋巴管浸润、低分化癌或肿瘤芽生的ECC患者,认为有必要进行更广泛的切除并伴有淋巴结清扫。即使病变通过内镜切除完全切除,对于低分化或中分化癌或淋巴管浸润的患者,也应考虑追加手术切除。