Dunlay Shannon M, Redfield Margaret M, Jiang Ruoxiang, Weston Susan A, Roger Véronique L
From the Division of Cardiovascular Diseases, Department of Medicine (S.M.D., M.M.R., V.L.R.) and Department of Health Sciences Research (S.M.D., R.J., S.A.W., V.L.R.), Mayo Clinic, Rochester, MN.
Circ Heart Fail. 2015 May;8(3):489-96. doi: 10.1161/CIRCHEARTFAILURE.114.001826. Epub 2015 Apr 1.
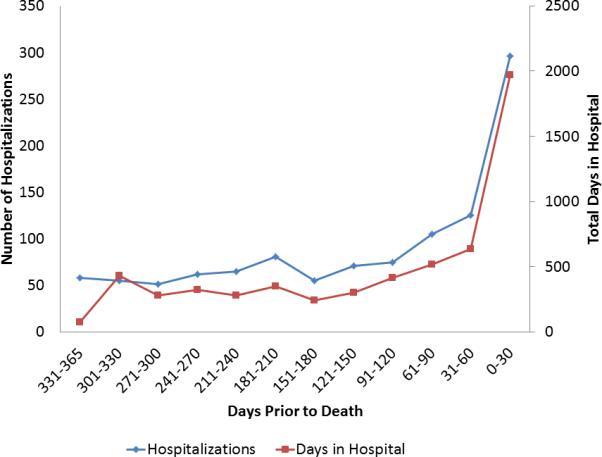
Healthcare utilization peaks at the end of life (EOL) in patients with heart failure. However, it is unclear what factors affect end of life utilization in patients with heart failure and if utilization has changed over time.
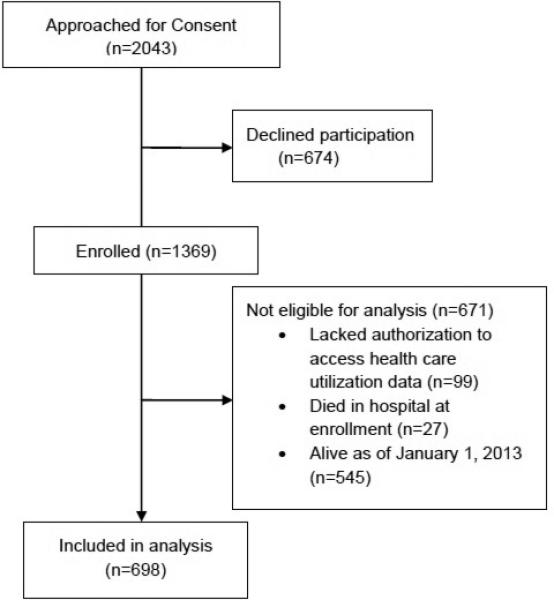
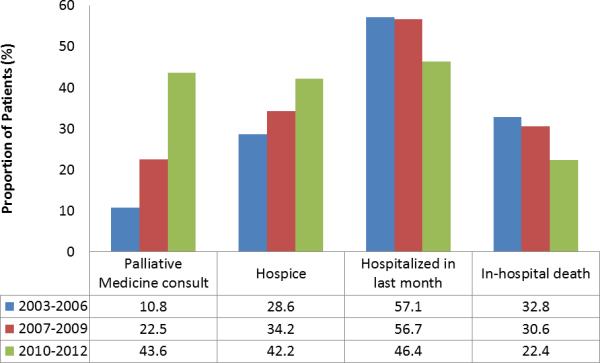
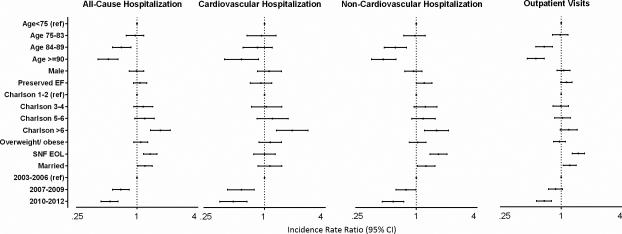
Southeastern Minnesota residents with heart failure were prospectively enrolled into a longitudinal cohort study from 2003 to 2011. Patients who died before December 31, 2012, were included in the analysis. Information on hospitalizations and outpatient visits in the last year of life was obtained using administrative sources. Negative binomial regression was used to assess the association between patient characteristics and utilization. The 698 decedents (47.3% men; 53.4% preserved ejection fraction) experienced 1528 hospitalizations (median 2 per person; range, 0-12; 37.6% because of cardiovascular causes) and 12 927 outpatient visits (median 14 per person; range, 0-119) in their last year of life. Most patients (81.5%) were hospitalized at least once and 28.4% died in the hospital. Patients who were older and those with dementia had lower utilization. Patients who were married, resided in a skilled nursing facility, and had more comorbidities had higher utilization. Patients with preserved ejection fraction had higher rates of noncardiovascular hospitalizations although other utilization was similar. Over time, rates of hospitalizations and outpatient visits decreased, whereas palliative care consults and enrollment in hospice increased.
Although patient factors remain associated with differential healthcare utilization at the end of life, utilization declined over time and use of palliative care services increased. These results are encouraging given the high resource use in patients with heart failure.
心力衰竭患者的医疗保健利用率在生命末期达到峰值。然而,尚不清楚哪些因素会影响心力衰竭患者生命末期的利用率,以及利用率是否随时间发生了变化。
2003年至2011年,明尼苏达州东南部的心力衰竭患者被前瞻性纳入一项纵向队列研究。纳入2012年12月31日前死亡的患者进行分析。利用行政资源获取生命最后一年的住院和门诊就诊信息。采用负二项回归评估患者特征与利用率之间的关联。698名死者(47.3%为男性;53.4%射血分数保留)在生命的最后一年经历了1528次住院(中位数每人2次;范围0 - 12次;37.6%因心血管原因)和12927次门诊就诊(中位数每人14次;范围0 - 119次)。大多数患者(81.5%)至少住院一次,28.4%在医院死亡。年龄较大和患有痴呆症的患者利用率较低。已婚、居住在专业护理机构且合并症较多的患者利用率较高。射血分数保留的患者非心血管住院率较高,尽管其他利用率相似。随着时间的推移,住院率和门诊就诊率下降,而姑息治疗咨询和临终关怀登记增加。
尽管患者因素仍然与生命末期不同的医疗保健利用率相关,但利用率随时间下降,姑息治疗服务的使用增加。鉴于心力衰竭患者资源使用量较高,这些结果令人鼓舞。