Xing Zhi-Heng, Sun Xin, Xu Long, Wu Qi, Li Li, Wu Xian-Jie, Shao Xu-Guang, Zhao Xin-Qian, Wang Jing-Hua, Ma Long-Yan, Wang Kai
Department of Respiratory, Tianjin Institute of Respiratory Diseases, Tianjin Haihe Hospital, Tianjin 300350, China.
Chin Med J (Engl). 2015 Apr 5;128(7):902-8. doi: 10.4103/0366-6999.154285.
The aim of this research was to evaluate long-term pulmonary sequelae on paired inspiration-expiration thin-section computed tomography (CT) scans 3 years after influenza A (H1N1) virus-associated pneumonia, and to analyze the affecting factors on pulmonary fibrosis.
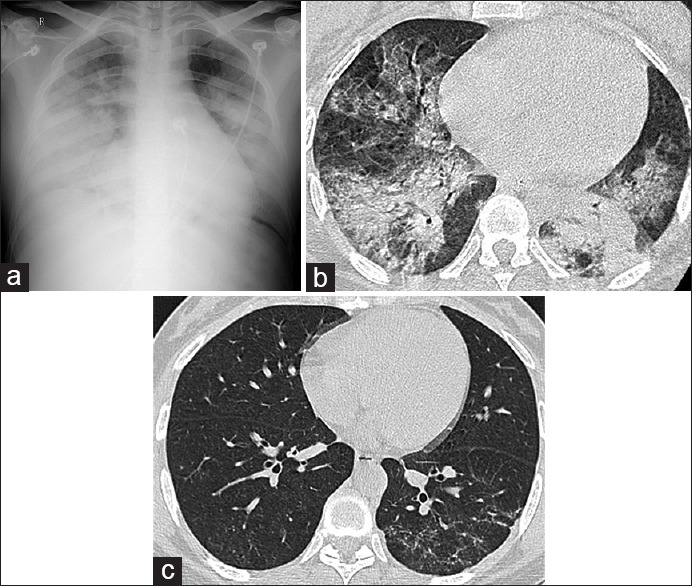
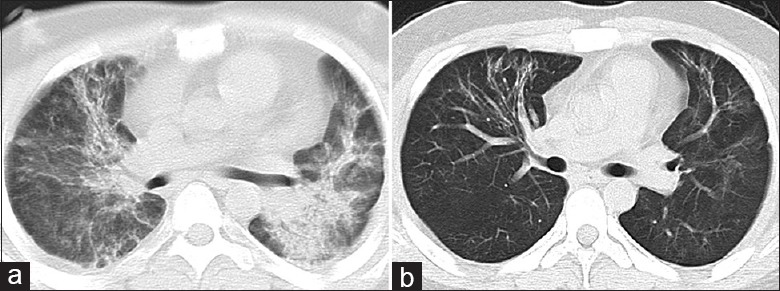
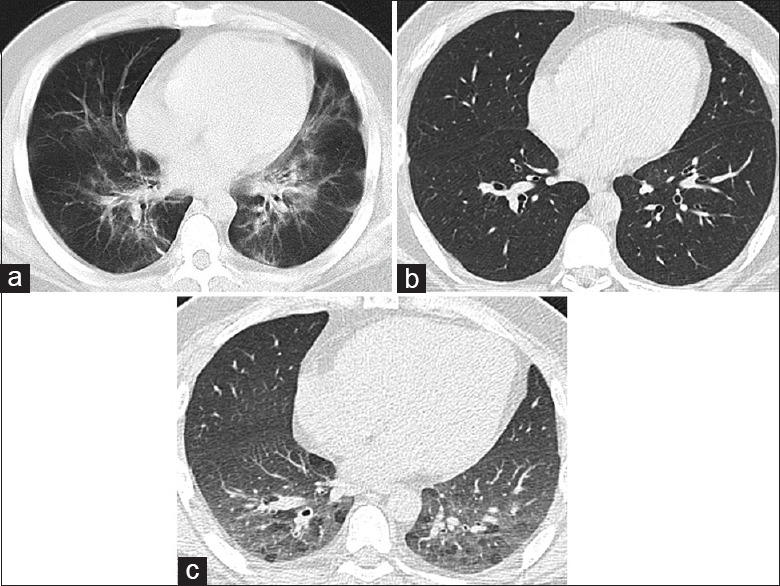
Twenty-four patients hospitalized with H1N1 virus-associated pneumonia at our hospital between September 2009 and January 2010 were included. The patients underwent thin-section CT 3 years after recovery. Abnormal pulmonary lesion patterns (ground-glass opacity, consolidation, parenchymal bands, air trapping, and reticulation) and evidence of fibrosis (architectural distortion, traction bronchiectasis, or honeycombing) were evaluated on follow-up thin-section CT. Patients were assigned to Group 1 (with CT evidence of fibrosis) and Group 2 (without CT evidence of fibrosis). Demographics, rate of mechanical ventilation therapy, rate of intensive care unit admission, cumulative prednisolone-equivalent dose, laboratory tests results (maximum levels of alanine aminotransferase, aspartate transaminase [AST], lactate dehydrogenase [LDH], and creatine kinase [CK]), and peak radiographic opacification of 24 patients during the course of their illness in the hospital were compared between two groups.
Parenchymal abnormality was present in 17 of 24 (70.8%) patients and fibrosis occurred in 10 of 24 (41.7%) patients. Patients in Group 1 (10/24; 41.7%) had a higher rate of mechanical ventilation therapy (Z = -2.340, P = 0.019), higher number of doses of cumulative prednisolone-equivalent (Z = -2.579, P = 0.010), higher maximum level of laboratory tests results (AST [Z = -2.140, P = 0.032], LDH [Z = -3.227, P = 0.001], and CK [Z = -3.345, P = 0.019]), and higher peak opacification on chest radiographs (Z = -2.743, P = 0.006) than patients in group 2 (14/24; 58.3%).
H1N1 virus-associated pneumonia frequently is followed by long-term pulmonary sequelae, including fibrotic changes, in lung parenchyma. Patients who need more steroid therapy, need more mechanical ventilation therapy, had higher laboratory tests results (maximum levels of AST, LDH, and CK), and had higher peak opacification on chest radiographs during treatment are more likely to develop lung fibrosis.
本研究旨在评估甲型H1N1流感病毒相关性肺炎3年后配对的吸气-呼气薄层计算机断层扫描(CT)上的长期肺部后遗症,并分析影响肺纤维化的因素。
纳入2009年9月至2010年1月期间在我院住院的24例甲型H1N1流感病毒相关性肺炎患者。患者康复3年后接受薄层CT检查。在随访的薄层CT上评估肺部异常病变模式(磨玻璃影、实变、实质条索、空气潴留和网状影)及纤维化证据(结构扭曲、牵拉性支气管扩张或蜂窝状改变)。将患者分为1组(CT有纤维化证据)和2组(CT无纤维化证据)。比较两组患者的人口统计学资料、机械通气治疗率、重症监护病房入住率、累积泼尼松等效剂量、实验室检查结果(丙氨酸氨基转移酶、天冬氨酸氨基转移酶[AST]、乳酸脱氢酶[LDH]和肌酸激酶[CK]的最高水平)以及24例患者在住院病程中的胸部X线片最大混浊度。
24例患者中有17例(70.8%)存在实质异常,24例中有10例(41.7%)发生纤维化。1组患者(10/24;41.7%)的机械通气治疗率更高(Z = -2.340,P = 0.019)、累积泼尼松等效剂量更多(Z = -2.579,P = 0.010)、实验室检查结果最高水平更高(AST[Z = -2.140,P = 0.032]、LDH[Z = -3.227,P = 0.001]和CK[Z = -3.345,P = 0.019]),且胸部X线片最大混浊度更高(Z = -2.743,P = 0.006),高于2组患者(14/24;58.3%)。
甲型H1N1流感病毒相关性肺炎常伴有长期肺部后遗症,包括肺实质的纤维化改变。需要更多激素治疗、需要更多机械通气治疗、实验室检查结果(AST、LDH和CK的最高水平)更高以及治疗期间胸部X线片最大混浊度更高的患者更易发生肺纤维化。