Cheng Xin, Liu Zhengcai, Liu Baoling, Zhao Ting, Li Yongqing, Alam Hasan B
Department of Surgery, University of Michigan Hospital, Ann Arbor, Michigan.
Department of Hepatobiliary Surgery, Xijing Hospital, The Fourth Military Medical University, Xi'an, China.
J Surg Res. 2015 Jul;197(1):39-44. doi: 10.1016/j.jss.2015.02.070. Epub 2015 Mar 6.
Hemorrhagic shock (HS) followed by a subsequent insult ("second hit") often initiates an exaggerated systemic inflammatory response and multiple organ failure. We have previously demonstrated that valproic acid, a pan histone deacetylase inhibitor, could improve survival in a rodent "two-hit" model. In the present study, our goal was to determine whether selective inhibition of histone deacetylase 6 with Tubastatin A (Tub-A) could prolong survival in a two-hit model where HS was followed by sepsis from cecal ligation and puncture (CLP).
C57Bl/6J mice were subjected to sublethal HS (30% blood loss) and then randomly divided into two groups (n = 13 per group) such as Tub-A group (treatment) and vehicle (VEH) group (control). The Tub-A group was given an intraperitoneal injection of Tub-A (70 mg/kg) dissolved in dimethyl sulfoxide (DMSO). The VEH group was injected with DMSO (1 μl/g body weight). After 24 h, all mice were subjected CLP followed immediately by another dose of Tub-A or DMSO. Survival was monitored for 10 d. In a parallel study, peritoneal irrigation fluid and liver tissue from Tub-A- or DMSO-treated mice were collected 3 h after CLP. Enzyme-linked immunosorbent assay was performed to quantify activity of the myeloperoxidase and concentrations of tumor necrosis factor-alpha (TNF-α) and interleukin 6 (IL-6) in the peritoneal irrigation fluid. RNA was isolated from the liver tissue, and real-time polymerase chain reaction was performed to measure relative messenger RNA levels of TNF-α and IL-6.
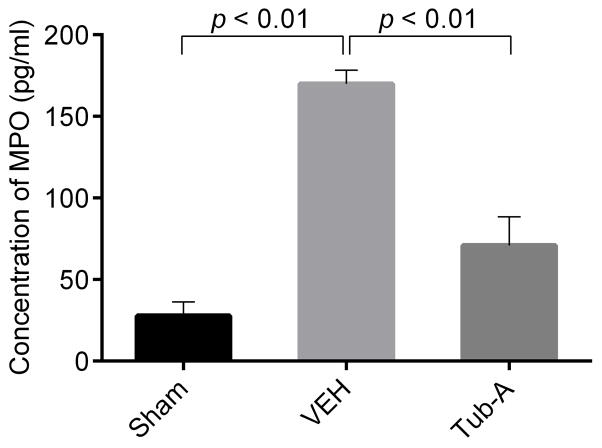
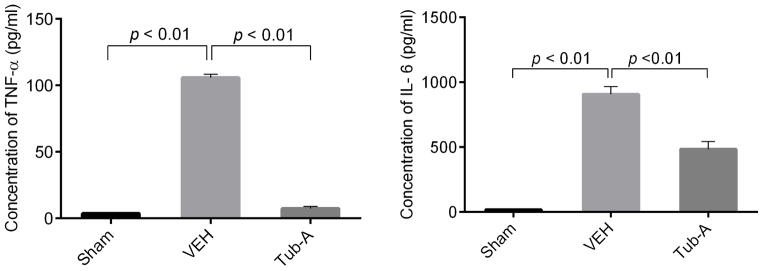
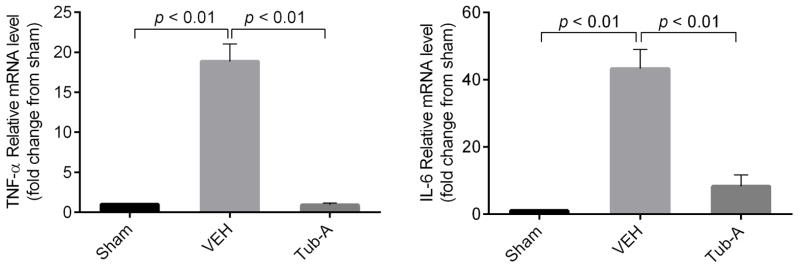
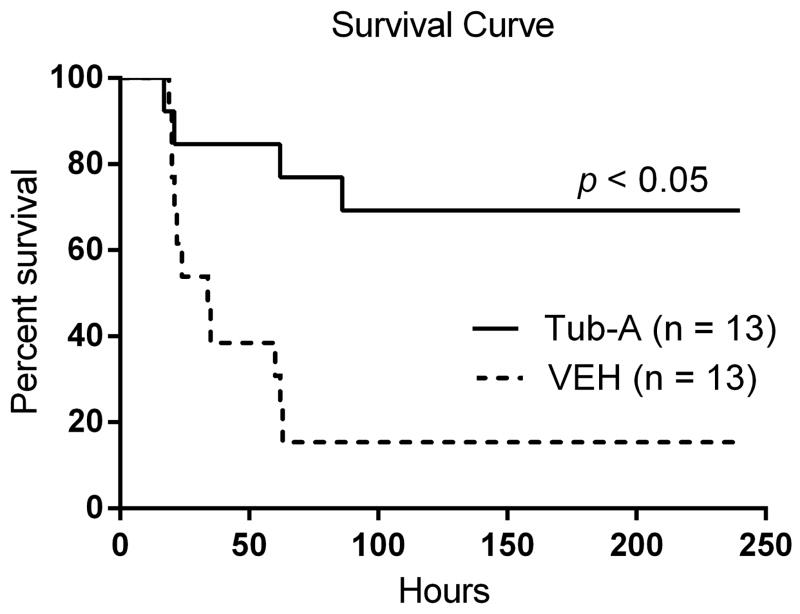
Treatment with Tub-A significantly improved survival compared with that of the control (69.2% versus 15.4%). In addition, Tub-A significantly suppressed myeloperoxidase activity (169.9 ± 8.4 ng/mL versus 70.4 ± 17.4 ng/mL; P < 0.01) and reduced levels of cytokines TNF-α and IL-6 in the peritoneal fluid (TNF-α: 105.7 ± 4.7 versus 7.4 ± 2.4 pg/mL; IL-6: 907.4 ± 2.3 versus 483.6 ± 1.6 pg/mL; P < 0.01) compared with those in the VEH control. Gene expression measured by real-time polymerase chain reaction confirmed that Tub-A inhibits transcription of TNF-α and IL-6.
Tub-A treatment significantly improves survival, attenuates inflammation, and downregulates TNF-α and IL-6 gene expression in a rodent two-hit model.
失血性休克(HS)后继发另一次损伤(“二次打击”)通常会引发过度的全身炎症反应和多器官功能衰竭。我们之前已经证明,一种泛组蛋白去乙酰化酶抑制剂丙戊酸,可提高啮齿动物“二次打击”模型的存活率。在本研究中,我们的目标是确定用Tubastatin A(Tub-A)选择性抑制组蛋白去乙酰化酶6是否能延长失血性休克后继发盲肠结扎穿孔(CLP)所致脓毒症的二次打击模型的存活时间。
对C57Bl/6J小鼠进行亚致死性失血性休克(失血30%),然后随机分为两组(每组n = 13),即Tub-A组(治疗组)和溶剂对照组(VEH组,对照组)。Tub-A组腹腔注射溶解于二甲基亚砜(DMSO)的Tub-A(70 mg/kg)。VEH组注射DMSO(1 μl/g体重)。24小时后,所有小鼠均接受CLP,随后立即给予另一剂量的Tub-A或DMSO。监测存活10天的情况。在一项平行研究中,CLP后3小时收集Tub-A或DMSO处理小鼠的腹腔灌洗液和肝组织。进行酶联免疫吸附测定以定量腹腔灌洗液中髓过氧化物酶的活性以及肿瘤坏死因子-α(TNF-α)和白细胞介素6(IL-6)的浓度。从肝组织中分离RNA,并进行实时聚合酶链反应以测量TNF-α和IL-6的相对信使RNA水平。
与对照组相比,Tub-A治疗显著提高了存活率(69.2%对15.4%)。此外,与VEH对照组相比,Tub-A显著抑制了髓过氧化物酶活性(169.9±8.4 ng/mL对70.4±17.4 ng/mL;P<0.01),并降低了腹腔液中细胞因子TNF-α和IL-6的水平(TNF-α:105.7±4.7对7.4±2.4 pg/mL;IL-6:907.4±2.3对483.6±1.6 pg/mL;P<0.01)。通过实时聚合酶链反应测量的基因表达证实,Tub-A抑制TNF-α和IL-6的转录。
在啮齿动物二次打击模型中,Tub-A治疗显著提高了存活率,减轻了炎症,并下调了TNF-α和IL-6基因的表达。