Sasse Michael, Dziuba Friederike, Jack Thomas, Köditz Harald, Kaussen Torsten, Bertram Harald, Beerbaum Philipp, Boehne Martin
Department of Pediatric Cardiology and Intensive Care Medicine, Hannover Medical School, Carl-Neuberg-Strasse 1, 30625, Hannover, Germany.
Pediatr Cardiol. 2015 Aug;36(6):1270-8. doi: 10.1007/s00246-015-1157-x. Epub 2015 Apr 7.
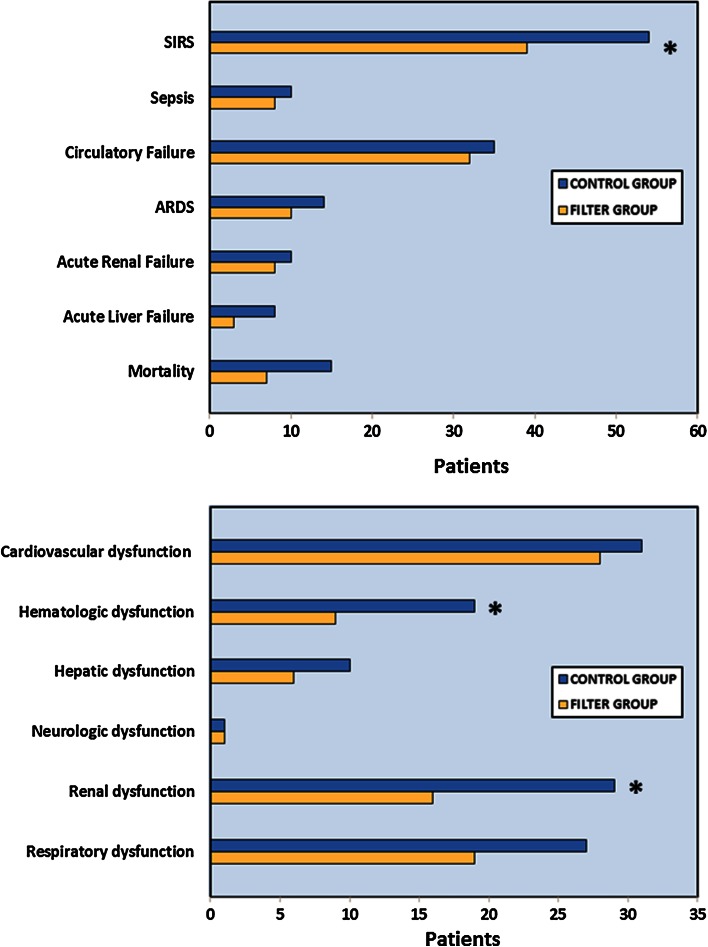
Cardiac surgery with cardiopulmonary bypass (CPB) frequently leads to systemic inflammatory response syndrome (SIRS) with concomitant organ malfunction. Infused particles may exacerbate inflammatory syndromes since they activate the coagulation cascade and alter inflammatory response or microvascular perfusion. In a randomized, controlled, prospective trial, we have previously shown that particle-retentive in-line filtration prevented major complications in critically ill children. Now, we investigated the effect of in-line filtration on major complications in the subgroup of cardiac patients. Children admitted to tertiary pediatric intensive care unit were randomized to either control or filter group obtaining in-line filtration throughout complete infusion therapy. Risk differences and 95 % confidence intervals (CI) of several complications such as SIRS, sepsis, mortality, various organ failure and dysfunction were compared between both groups using the Wald method. 305 children (n = 150 control, n = 155 filter group) with cardiac diseases were finally analyzed. The majority was admitted after cardiac surgery with CPB. Risk of SIRS (-11.3 %; 95 % CI -21.8 to -0.5 %), renal (-10.0 %; 95 % CI -17.0 to -3.0 %) and hematologic (-8.1 %; 95 % CI -14.2 to -0.2 %) dysfunction were significantly decreased within the filter group. No risk differences were demonstrated for occurrence of sepsis, any other organ failure or dysfunctions between both groups. Infused particles might aggravate a systemic hypercoagulability and inflammation with subsequent organ malfunction in pediatric cardiac intensive care patients. Particle-retentive in-line filtration might be effective in preventing SIRS and maintaining renal and hematologic function. In-line filtration offers a novel therapeutic option to decrease morbidity in cardiac intensive care.
体外循环(CPB)心脏手术常导致全身炎症反应综合征(SIRS)并伴有器官功能障碍。注入的微粒可能会加剧炎症综合征,因为它们会激活凝血级联反应并改变炎症反应或微血管灌注。在一项随机、对照、前瞻性试验中,我们先前已表明,颗粒截留式在线过滤可预防危重症儿童的主要并发症。现在,我们研究了在线过滤对心脏病患者亚组主要并发症的影响。入住三级儿科重症监护病房的儿童被随机分为对照组或过滤组,在整个输液治疗过程中进行在线过滤。使用Wald方法比较两组之间几种并发症(如SIRS、脓毒症、死亡率、各种器官衰竭和功能障碍)的风险差异和95%置信区间(CI)。最终分析了305例患有心脏病的儿童(n = 150例对照组,n = 155例过滤组)。大多数儿童是在CPB心脏手术后入院的。过滤组中SIRS(-11.3%;95%CI -21.8至-0.5%)、肾脏(-10.0%;95%CI -17.0至-3.0%)和血液学(-8.1%;95%CI -14.2至-0.2%)功能障碍的风险显著降低。两组之间在脓毒症、任何其他器官衰竭或功能障碍的发生方面未显示出风险差异。注入的微粒可能会加重小儿心脏重症监护患者的全身高凝状态和炎症,随后导致器官功能障碍。颗粒截留式在线过滤可能有效地预防SIRS并维持肾脏和血液学功能。在线过滤为降低心脏重症监护中的发病率提供了一种新的治疗选择。