Assistance Publique-Hôpitaux de Paris, Neonatal intensive care unit, Robert Debré children's hospital, Paris, France.
Delegation Paris 7, Inserm U1141, University of Paris, Paris, France.
Sci Rep. 2020 Mar 19;10(1):5003. doi: 10.1038/s41598-020-61815-4.
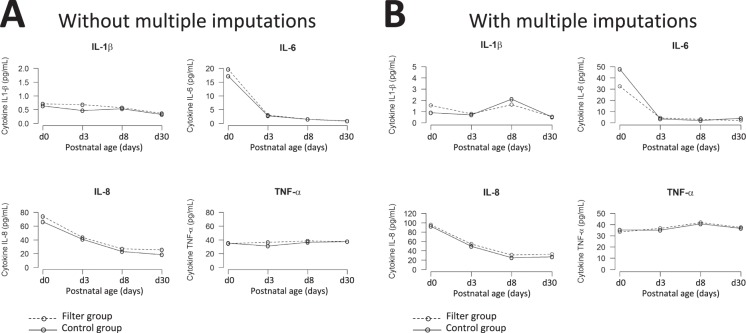
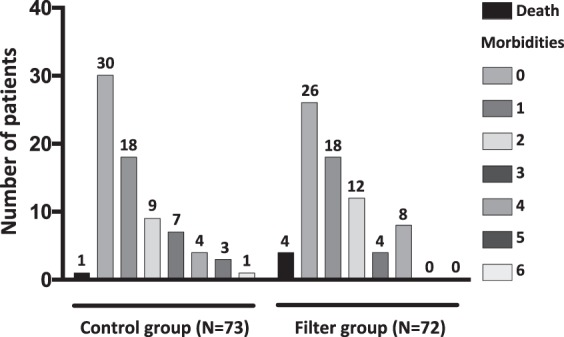
In-line filtration is increasingly used in critically-ill infants but its benefits, by preventing micro-particle infusion in very preterm neonates, remain to be demonstrated. We conducted a randomized controlled trial among very preterm infants allocated to receive either in-line filtration of all the intra-venous lines or standard care without filters. The primary outcome was differences greater than 20% in the median changes in pro-inflammatory cytokine serum concentrations measured at day 3 and day 8 (+/-1) using a Luminex multianalytic profiling technique. Major neonatal complications were analyzed as secondary predefined outcomes. We randomized 146 infants, assigned to filter (n = 73) or control (n = 73) group. Difference over 20% in pro-inflammatory cytokine concentration between day 3 and day 8 was not found statistically different between the two groups, both in intent-to-treat (with imputation) and per protocol (without imputation) analyses. The incidences of most of neonatal complications were found to be similar. Hence, this trial did not evidence a beneficial effect of in-line filtration in very preterm infants on the inflammatory response syndrome and neonatal morbidities. These data should be interpreted according to local standards in infusion preparation and central line management.
在线过滤在危重新生儿中越来越多地被使用,但通过防止极早产儿静脉输注微颗粒,其益处仍有待证明。我们在极早产儿中进行了一项随机对照试验,将他们分为接受所有静脉输液线在线过滤的组或不使用过滤器的标准护理组。主要结局是使用 Luminex 多分析谱技术测量第 3 天和第 8 天(+/-1)的促炎细胞因子血清浓度的中位数变化差异大于 20%。主要新生儿并发症被分析为次要预定结局。我们随机分配了 146 名婴儿,分为过滤组(n=73)或对照组(n=73)。在意向治疗(有插补)和方案(无插补)分析中,两组之间第 3 天和第 8 天之间促炎细胞因子浓度的差异超过 20%,均无统计学差异。大多数新生儿并发症的发生率相似。因此,本试验并未证明在线过滤对极早产儿炎症反应综合征和新生儿发病率有有益影响。这些数据应根据当地输液准备和中心静脉管理标准进行解释。