Hodgson David, Anderson John, Reynolds Catherine, Meakin Garry, Bailey Helen, Pavord Ian, Shaw Dominick, Harrison Tim
Nottingham Respiratory Research Unit, University of Nottingham, Nottingham, UK.
Nuffield Department of Medicine, University of Oxford, Oxford, UK.
Thorax. 2015 Jun;70(6):559-65. doi: 10.1136/thoraxjnl-2014-206481. Epub 2015 Apr 9.
Some patients with refractory asthma have evidence of uncontrolled eosinophilic inflammation in the distal airways. While traditional formulations of inhaled steroids settle predominantly in the large airways, newer formulations with an extra-fine particle size have a more peripheral pattern of deposition. Specifically treating distal airway inflammation may improve asthma control.
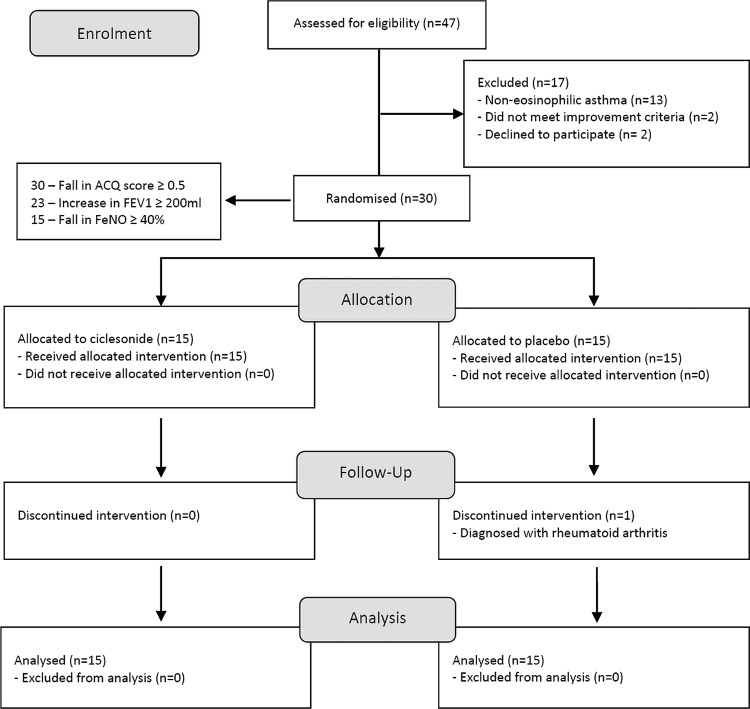
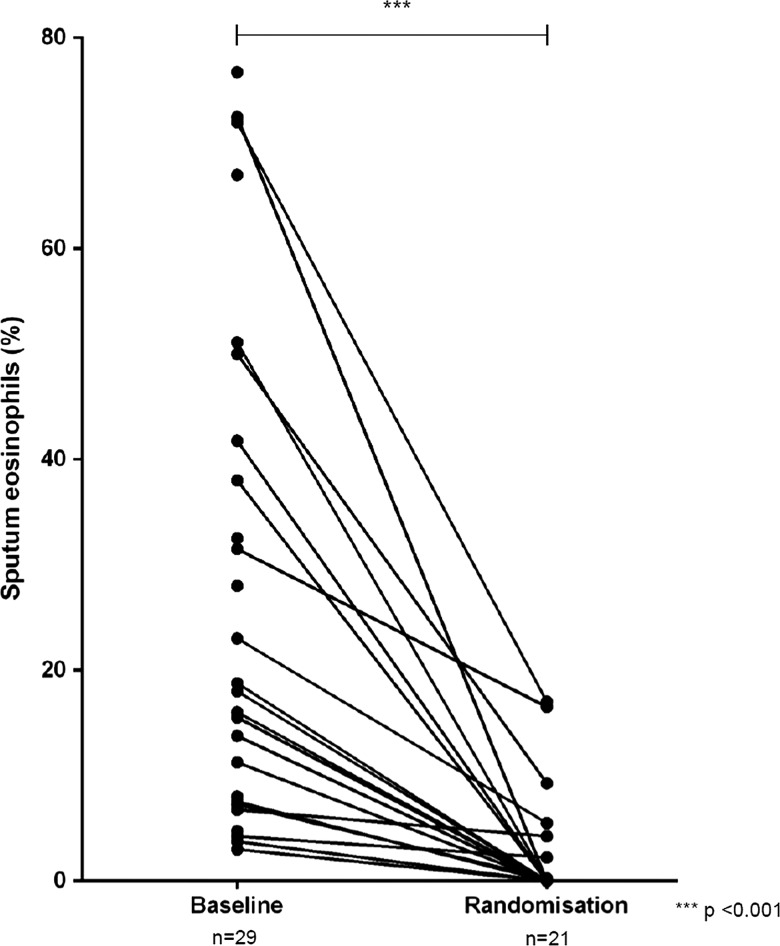
30 patients with refractory asthma despite high dose inhaled corticosteroids were identified as having persistent airway eosinophilia. Following 2 weeks of prednisolone 30 mg, patients demonstrating an improvement in asthma control were randomised to receive either ciclesonide 320 µg twice daily or placebo in addition to usual maintenance therapy for 8 weeks. The primary outcome measure was sputum eosinophil count at week 8. Alveolar nitric oxide was measured as a marker of distal airway inflammation.
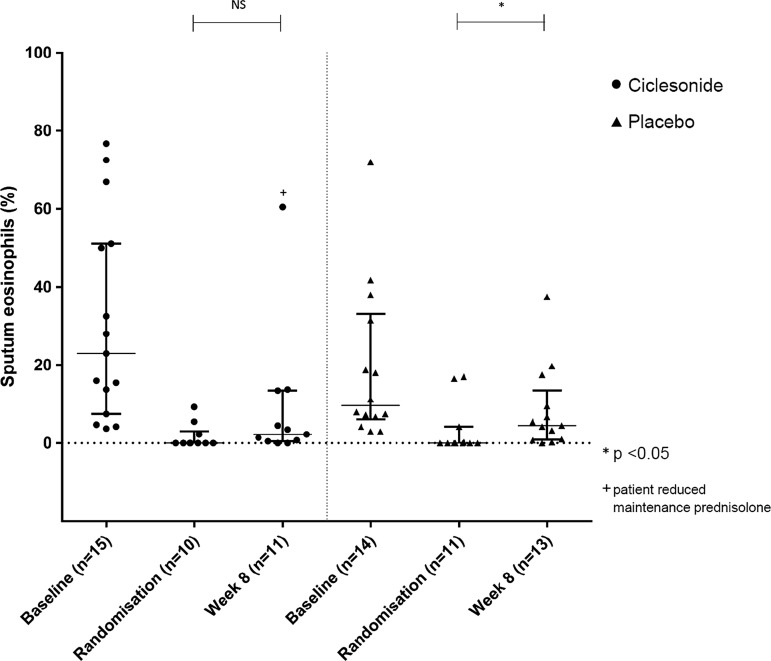
There was continued suppression of differential sputum eosinophil counts with ciclesonide (median 2.3%) but not placebo (median 4.5%) though the between-group difference was not significant. When patients who had changed their maintenance prednisolone dose during the trial were excluded the difference between groups was significant (1.4% vs 4.5%, p=0.028). Though alveolar nitric oxide decreased with ciclesonide the value did not reach statistical significance.
These data demonstrate that patients with ongoing eosinophilic inflammation are not truly refractory, and that suppression of airway eosinophilia may be maintained with additional inhaled corticosteroid. Further work is needed with a focus on patient-orientated outcome measures such as exacerbation rate, with additional tests of small airway function.
NCT01171365. Protocol available at http://www.clinicaltrials.gov.
一些难治性哮喘患者存在远端气道嗜酸性粒细胞炎症未得到控制的证据。传统剂型的吸入性糖皮质激素主要沉积在大气道,而新型的超细微粒剂型则具有更外周的沉积模式。特异性治疗远端气道炎症可能改善哮喘控制。
30例尽管使用高剂量吸入性糖皮质激素仍为难治性哮喘的患者被确定为存在持续性气道嗜酸性粒细胞增多。在接受2周30mg泼尼松龙治疗后,哮喘控制得到改善的患者被随机分组,除常规维持治疗外,分别接受每日两次320μg环索奈德或安慰剂治疗8周。主要结局指标为第8周时的痰液嗜酸性粒细胞计数。测量肺泡一氧化氮作为远端气道炎症的标志物。
环索奈德组痰液嗜酸性粒细胞分类计数持续受到抑制(中位数2.3%),而安慰剂组未受抑制(中位数4.5%),尽管组间差异无统计学意义。排除试验期间改变维持泼尼松龙剂量的患者后,两组间差异有统计学意义(1.4%对4.5%,p = 0.028)。尽管环索奈德使肺泡一氧化氮降低,但该值未达到统计学意义。
这些数据表明,持续存在嗜酸性粒细胞炎症的患者并非真正难治,额外吸入糖皮质激素可维持气道嗜酸性粒细胞增多的抑制。需要进一步开展工作,重点关注以患者为导向的结局指标,如加重率,并进行额外的小气道功能测试。
NCT01171365。方案可在http://www.clinicaltrials.gov获取。