Kimmel Lara A, Wilson Scott, Janardan Jyotsna D, Liew Susan M, Walker Rowan G
Department of Physiotherapy , The Alfred Hospital , Melbourne , Australia ; Department of Epidemiology and Preventive Medicine , Monash University , Melbourne , Australia.
Department of Renal Medicine , The Alfred Hospital , Melbourne , Australia ; Baker IDI , Melbourne , Australia.
Clin Kidney J. 2014 Dec;7(6):546-51. doi: 10.1093/ckj/sfu108. Epub 2014 Oct 28.
Total joint arthroplasty (TJA) is a common procedure with demand for arthroplasties expected to increase exponentially. Incidence of acute kidney injury (AKI) following TJA is reportedly low, with most studies finding an incidence of <2%, increasing to 9% when emergency orthopaedic patients are included.
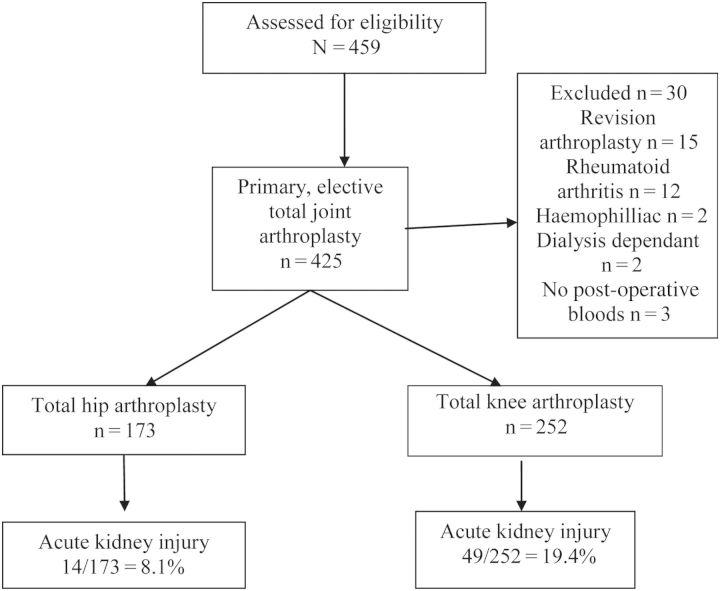
Retrospective medical record review of consecutive primary, elective TJA procedures was undertaken at a large tertiary hospital (Alfred). Demographic, peri-operative and post-operative data were recorded. Factors associated with AKI (based on RIFLE criteria) were determined using multiple logistic regression.
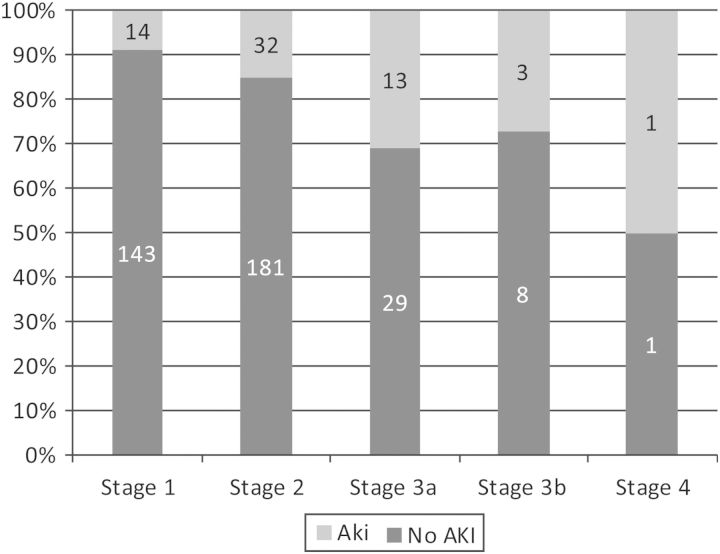
Between January 2011 and June 2013, 425 patients underwent TJA; 252 total knee replacements (TKR) and 173 total hip replacements (THR). Sixty-seven patients (14.8%) developed AKI, including 51 TKR. Factors associated with AKI (adjusting for known confounders) include increasing body mass index [adjusted odds ratio (AOR) 1.14; 95% CI: 1.07, 1.21], older age (AOR 1.07; 95% CI 1.02, 1.13) and lower pre-operative glomerular filtration rate (AOR 0.97; 95% CI 0.96, 0.99) and taking angiotensin-converting enzyme inhibitors (AOR 2.70; 95% CI 1.12, 6.48) and angiotensin-II receptor blockers (AOR 2.64; 95% CI 1.18, 5.93). In most patients, AKI resolved by discharge, however, only 62% of patients had renal function tests after discharge.
This study showed a rate of AKI of nearly 15% in our TJA population, substantially higher than previously reported. Given that AKI and long-term complications are associated, prospective research is needed to further understand the associated factors and predict those at risk of AKI. There may be opportunities to maximize the pre-operative medical management and mitigate risk.
全关节置换术(TJA)是一种常见的手术,预计关节置换术的需求将呈指数级增长。据报道,TJA后急性肾损伤(AKI)的发生率较低,大多数研究发现发生率<2%,若纳入急诊骨科患者,发生率则升至9%。
在一家大型三级医院(阿尔弗雷德医院)对连续进行的初次择期TJA手术进行回顾性病历审查。记录人口统计学、围手术期和术后数据。使用多因素逻辑回归确定与AKI相关的因素(基于RIFLE标准)。
2011年1月至2013年6月期间,425例患者接受了TJA;其中252例为全膝关节置换术(TKR),173例为全髋关节置换术(THR)。67例患者(14.8%)发生了AKI,其中51例为TKR。与AKI相关的因素(校正已知混杂因素后)包括体重指数增加[校正比值比(AOR)1.14;95%置信区间:1.07,1.21]、年龄较大(AOR 1.07;95%置信区间1.02,1.13)、术前肾小球滤过率较低(AOR 0.97;95%置信区间0.96,0.99)以及服用血管紧张素转换酶抑制剂(AOR 2.70;95%置信区间1.12,6.48)和血管紧张素II受体阻滞剂(AOR 2.64;95%置信区间1.18,5.93)。大多数患者在出院时AKI得到缓解,然而,只有62%的患者在出院后进行了肾功能检查。
本研究显示,在我们的TJA患者群体中,AKI发生率接近15%,大大高于先前报道的发生率。鉴于AKI与长期并发症相关,需要进行前瞻性研究以进一步了解相关因素并预测有AKI风险的患者。可能有机会优化术前医疗管理并降低风险。