Xia Hui, Wang Xiaomen, Li Fabin, Longuet Christophe, Vernet Guy, Goletti Delia, Zhao Yanlin, Lagrange Philippe H
National Tuberculosis Reference Laboratory, Chinese Center for Disease Control and Prevention, Beijing, People's Republic of China.
Tuberculosis Control Center of Heilongjiang Province, Harbin, Heilongjiang, People's Republic of China.
PLoS One. 2015 Apr 13;10(4):e0121021. doi: 10.1371/journal.pone.0121021. eCollection 2015.
Interferon-release assays (IGRAs) for diagnosing active pulmonary tuberculosis (PTB) are not yet fully validated, particularly in high TB-endemic areas as the People's Republic of China (PRC). The aim of this report was to assess the performance of the QuantiFERON-TB Gold In-tube (QFT-GIT) and tuberculin skin test (TST), in addition to microbiological results, as contributors for diagnosing active PTB in the PRC.
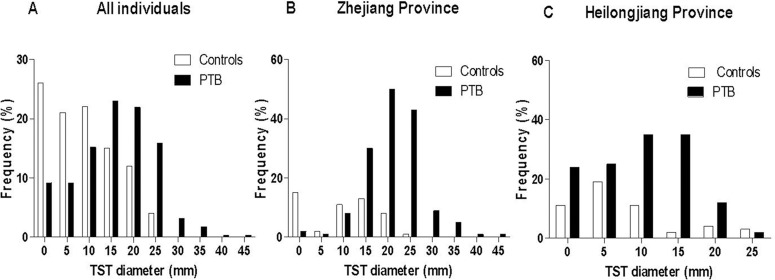
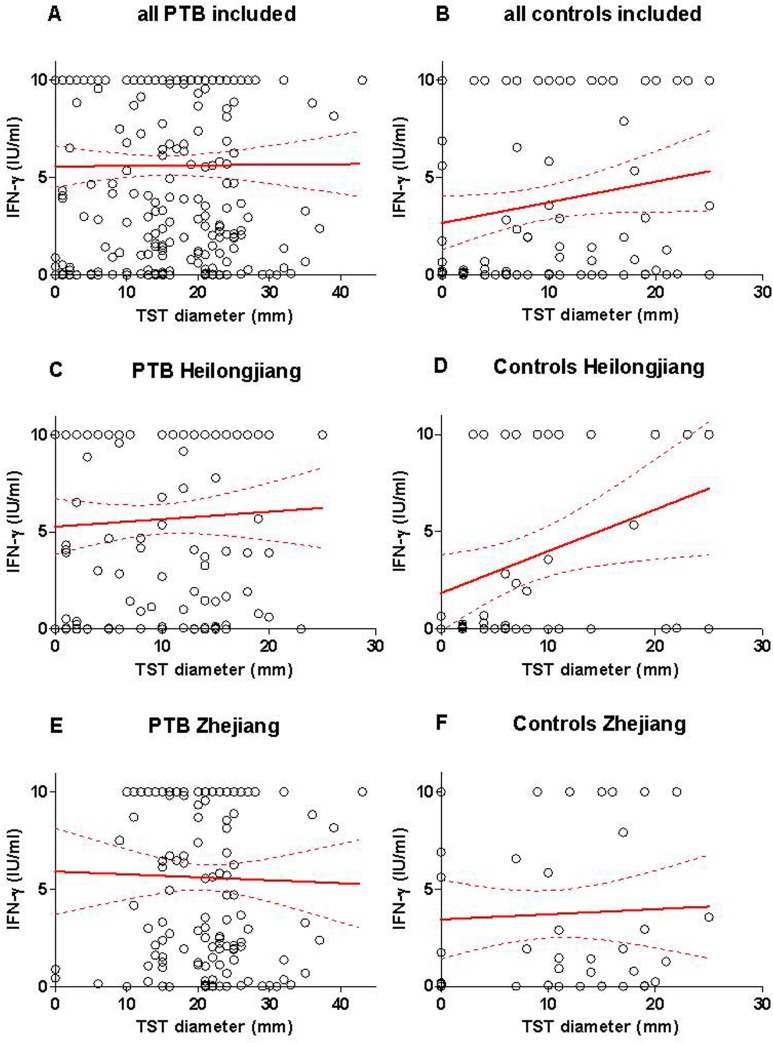
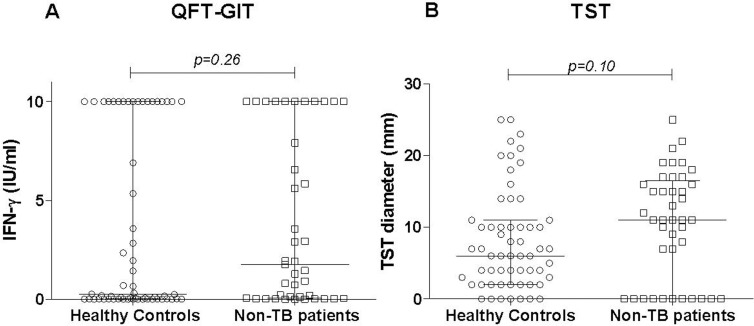
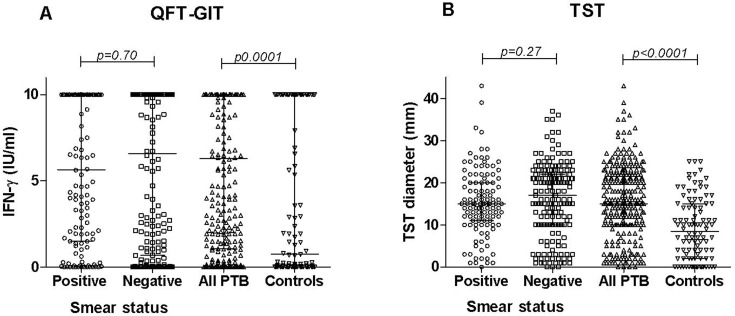
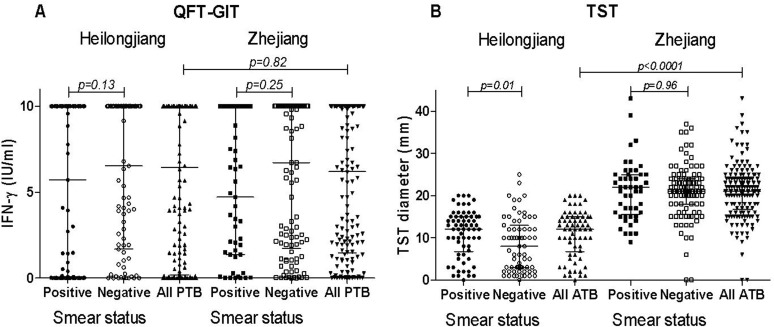
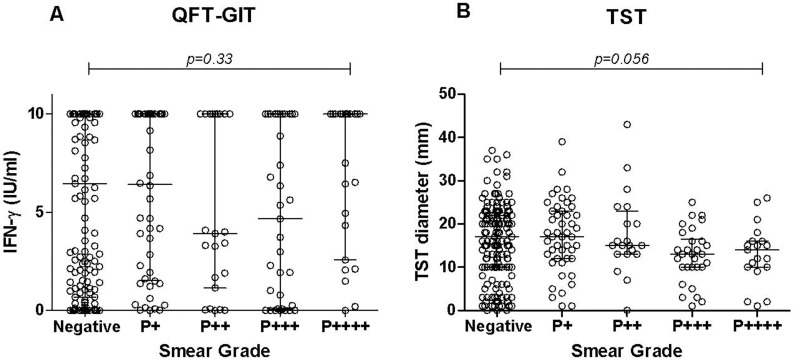
METHODS/PRINCIPAL FINDINGS: A total of 300 PTB patients, 41 disease controls (DC) and 59 healthy community controls (HCC) were included prospectively between May 2010 and April 2011 from two provinces of the PRC (Heilongjiang and Zhejiang). The QFT-GIT and TST yielded an overall sensitivity for active TB of 80.9% and 86.2%, and a specificity of 36.6% and 26.8%, respectively. The province of origin and smear microscopy status did not significantly impact the diagnostic values for PTB. However, using the TST with a 10 mm cut-off point, a significantly higher proportion of LTBI was observed in the DC than the HCC (p=0.01). Discordant results between the QFT-GIT and TST were found among 1/3 of the PTB, HCC and DC. Two-thirds of the individuals presented TST-positive/QFT-GIT-negative discordant results. The TST-negative/QFT-GIT-positive result was not associated with age or bacillary load. Cumulative QFT-GIT and TST positive results increased the overall sensitivity (95.9%), but it was associated with a dramatic decrease of the overall specificity (24.8%) leading to a suboptimal PPV (80.1%) and a low NPV (61.1%).
CONCLUSIONS/SIGNIFICANCE: The usefulness of the QFT-GIT to diagnose active TB in high TB-endemic countries remains doubtful because like the TST, the QFT-GIT cannot distinguish between LTBI and active TB. Used as single stand-alone tests, both the QFT-GIT and TST have very limited roles in the diagnosis of active PTB. However, the combined use of SM, the TST and QFT-GIT may allow for the exclusion of ATB.
用于诊断活动性肺结核(PTB)的干扰素释放检测(IGRAs)尚未得到充分验证,尤其是在结核病高流行地区,如中华人民共和国(中国)。本报告的目的是评估管内QuantiFERON-TB Gold(QFT-GIT)和结核菌素皮肤试验(TST)以及微生物学检测结果在中国诊断活动性PTB中的作用。
方法/主要发现:2010年5月至2011年4月期间,在中国的两个省份(黑龙江和浙江)前瞻性纳入了300例PTB患者、41例疾病对照(DC)和59例健康社区对照(HCC)。QFT-GIT和TST对活动性结核病的总体敏感性分别为80.9%和86.2%,特异性分别为36.6%和26.8%。患者的籍贯和涂片显微镜检查结果对PTB的诊断价值没有显著影响。然而,以10mm为切点使用TST时,DC中潜伏性结核感染(LTBI)的比例显著高于HCC(p=0.01)。在三分之一的PTB患者、HCC和DC中发现QFT-GIT和TST结果不一致。三分之二的个体表现为TST阳性/QFT-GIT阴性的不一致结果。TST阴性/QFT-GIT阳性结果与年龄或菌量无关。QFT-GIT和TST的累积阳性结果提高了总体敏感性(95.9%),但与总体特异性的显著降低(24.8%)相关,导致阳性预测值(PPV)不理想(80.1%)和阴性预测值(NPV)较低(61.1%)。
结论/意义:QFT-GIT在结核病高流行国家诊断活动性结核病的实用性仍然存疑,因为与TST一样,QFT-GIT无法区分LTBI和活动性结核病。作为单独的检测方法,QFT-GIT和TST在诊断活动性PTB方面的作用非常有限。然而,痰涂片镜检(SM)、TST和QFT-GIT联合使用可能有助于排除活动性结核病(ATB)。