Michalow Julia, Chola Lumbwe, McGee Shelley, Tugendhaft Aviva, Pattinson Robert, Kerber Kate, Hofman Karen
Priority Cost-Effective Lessons for Systems Strengthening-South Africa (PRICELESS SA), Medical Research Council/Wits Rural Public Health and Health Transition Research Unit (Agincourt), Johannesburg, South Africa.
School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, 27 St Andrews Road, Parktown, 2193, Johannesburg, South Africa.
BMC Pregnancy Childbirth. 2015 Feb 18;15:39. doi: 10.1186/s12884-015-0456-9.
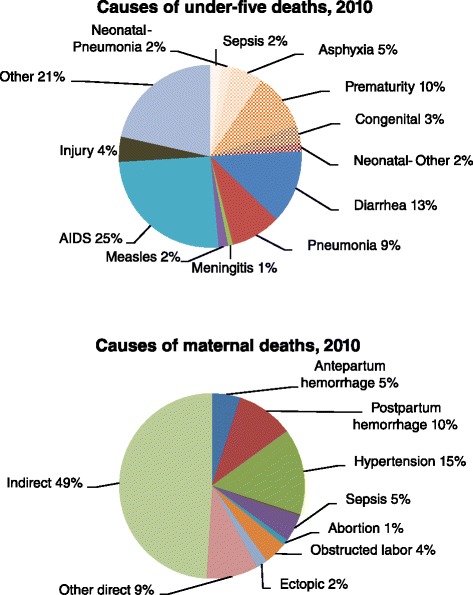
The time of labor, birth and the first days of life are the most vulnerable period for mothers and children. Despite significant global advocacy, there is insufficient understanding of the investment required to save additional lives. In particular, stillbirths have been neglected. Over 20 000 stillbirths are recorded annually in South Africa, many of which could be averted. This analysis examines available South Africa specific stillbirth data and evaluates the impact and cost-effectiveness of 13 interventions acknowledged to prevent stillbirths and maternal and newborn mortality.
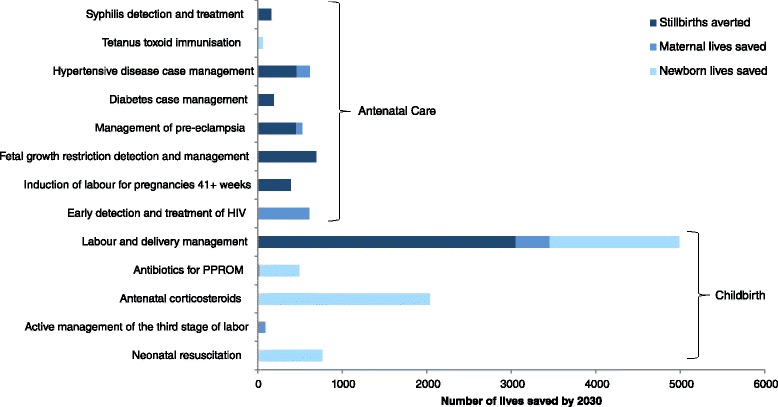
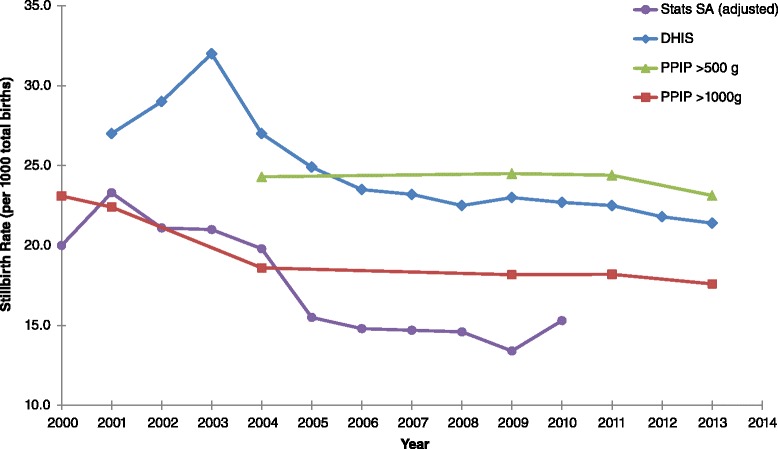
Multiple data sources were reviewed to evaluate changes in stillbirth rates since 2000. The intervention analysis used the Lives Saved tool (LiST) and the Family Planning module (FamPlan) in Spectrum. LiST was used to determine the number of stillbirths and maternal and neonatal deaths that could be averted by scaling up the interventions to full coverage (99%) in 2030. The impact of family planning was assessed by increasing FamPlan's default 70% coverage of modern contraception to 75% and 80% coverage. Total and incremental costs were determined in the LiST costing module. Cost-effectiveness measured incremental cost effectiveness ratios per potential life years gained.
Significant variability exists in national stillbirth data. Using the international stillbirth definition, the SBR was 17.6 per 1 000 births in 2013. Full coverage of the 13 interventions in 2030 could reduce the SBR by 30% to 12.4 per 1 000 births, leading to an MMR of 132 per 100 000 and an NMR of 7 per 1 000 live births. Increased family planning coverage reduces the number of deaths significantly. The full intervention package, with 80% family planning coverage in 2030, would require US$420 million (US$7.8 per capita) annually, which is less than baseline costs of US$550 million (US$10.2 per capita). All interventions were highly cost-effective.
This is the first analysis in South Africa to assess the impact of scaling up interventions to avert stillbirths. Improved coverage of 13 interventions that are already recommended could significantly impact the rates of stillbirth and maternal and neonatal mortality. Family planning should also be prioritized to reduce mortality and overall costs.
分娩期、出生时及出生后的头几天是母亲和儿童最脆弱的时期。尽管全球大力倡导,但对于拯救更多生命所需的投入仍缺乏足够的认识。特别是死产问题一直被忽视。南非每年记录的死产超过20000例,其中许多是可以避免的。本分析研究了南非特有的现有死产数据,并评估了13种公认可预防死产及孕产妇和新生儿死亡的干预措施的影响和成本效益。
回顾了多个数据源,以评估2000年以来死产率的变化。干预分析使用了Lives Saved工具(LiST)和Spectrum中的计划生育模块(FamPlan)。LiST用于确定通过在2030年将干预措施扩大到全面覆盖(99%)可避免的死产数以及孕产妇和新生儿死亡数。通过将FamPlan中现代避孕方法的默认覆盖率从70%提高到75%和80%来评估计划生育的影响。在LiST成本核算模块中确定总成本和增量成本。成本效益以每获得一个潜在生命年的增量成本效益比来衡量。
全国死产数据存在显著差异。根据国际死产定义,2013年死产率为每1000例出生17.6例。2030年对13种干预措施的全面覆盖可将死产率降低30%,降至每1000例出生12.4例,导致孕产妇死亡率为每10万例132例,新生儿死亡率为每1000例活产7例。提高计划生育覆盖率可显著减少死亡人数。2030年计划生育覆盖率达到80%的全面干预方案每年需要4.2亿美元(人均7.8美元),低于5.5亿美元(人均10.2美元)的基线成本。所有干预措施都具有很高的成本效益。
这是南非首次评估扩大干预措施以避免死产的影响。提高已推荐的13种干预措施的覆盖率可显著影响死产率以及孕产妇和新生儿死亡率。还应优先考虑计划生育,以降低死亡率和总体成本。