Tazzari Marcella, Palassini Elena, Vergani Barbara, Villa Antonello, Rini Francesca, Negri Tiziana, Colombo Chiara, Crippa Flavio, Morosi Carlo, Casali Paolo G, Pilotti Silvana, Stacchiotti Silvia, Rivoltini Licia, Castelli Chiara
Department of Experimental Oncology and Molecular Medicine, Unit of Immunotherapy of Human Tumours, Milan, Italy.
Fondazione IRCCS Istituto Nazionale dei Tumori, Via G. Venezian 1, Milan, 20133, Italy.
BMC Cancer. 2015 Feb 14;15:58. doi: 10.1186/s12885-015-1044-0.
Clear cell sarcoma (CCS), initially named malignant melanoma of soft parts, is an aggressive soft tissue sarcoma (STS) that, due to MITF activation, shares with melanoma the expression of melanocyte differentiation antigens. CCS is poorly sensitive to chemotherapy. Multi-kinase inhibitors have been used as therapeutic agents. In the case we report here, treatment with sunitinib induced a long-lasting clinical response that was associated with an immune activation directed against Melan-A/MART-1 antigen.
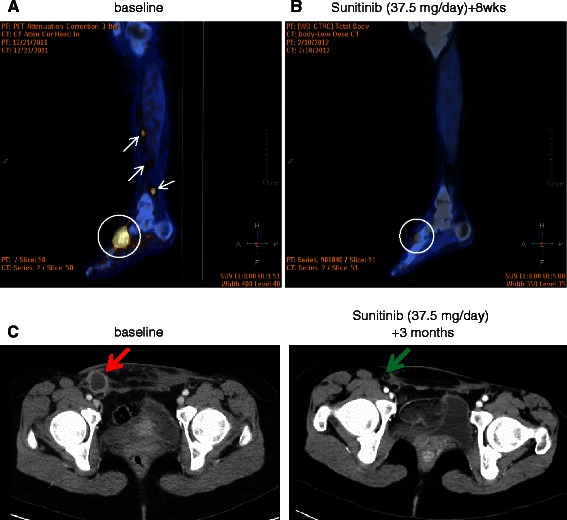
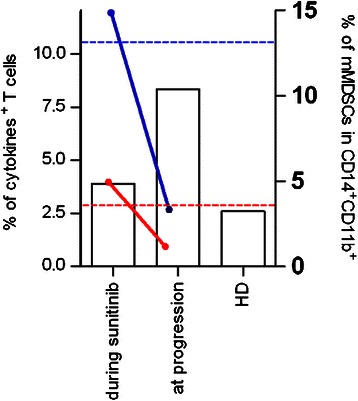
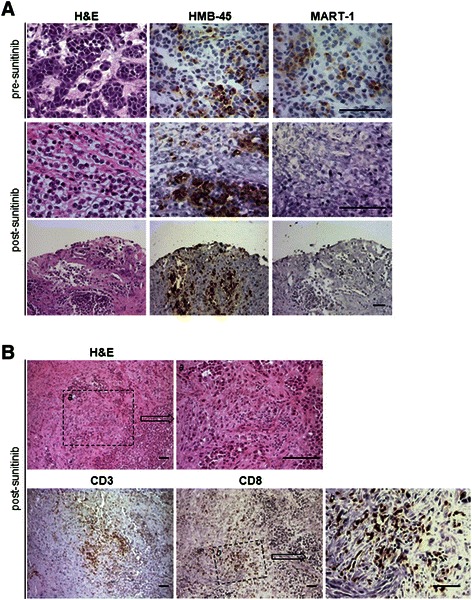
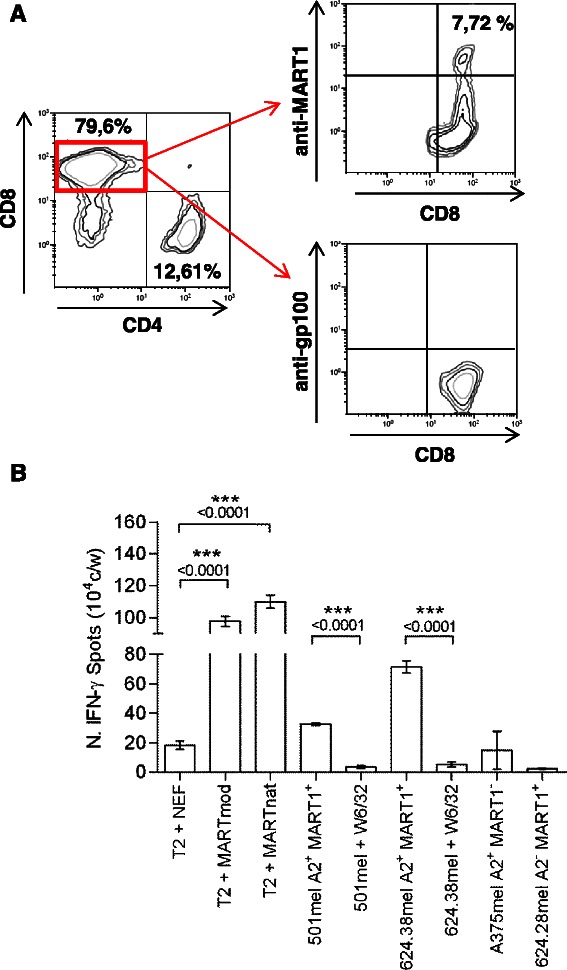
A 28 years old female patient with an advanced molecularly confirmed CCS resistant to conventional chemotherapy was started in January 2012 on sunitinib, 37.5 mg/day, with evidence of radiologic and metabolic response at the primary and metastatic sites of disease. Pathologic response and loss of the Melan-A/MART-1 antigen were evidenced on residual tumor removed in April 2012. Immunological monitoring performed on patient's blood during pharmacological treatment revealed a systemic, Melan-A/MART-1 specific immunity and a low frequency of immunosuppressive cells. Sunitinib was restarted in May 2012, with a new response, and continued for 11 months although with repeatedly interruptions due to toxicity. Disease progression and new responses were documented at each treatment interruption and restart. Sunitinib was definitively interrupted in April 2013 for disease progression.
The analysis of this case proves that antigens expressed by CCS, as for melanoma, can be immunogenic in vivo and that tumor-antigen specific T cells may exert anti-tumor activity in CCS patient. Thus, manipulation of the immune response may have therapeutic potential for this STS subtype and immunotherapy approaches, can be promising therapeutic options for these patients.
透明细胞肉瘤(CCS)最初被命名为软组织恶性黑色素瘤,是一种侵袭性软组织肉瘤(STS),由于MITF激活,与黑色素瘤共享黑素细胞分化抗原的表达。CCS对化疗敏感性较差。多激酶抑制剂已被用作治疗药物。在我们报道的这个病例中,舒尼替尼治疗诱导了持久的临床反应,这与针对Melan-A/MART-1抗原的免疫激活有关。
一名28岁的女性患者,经分子确诊为晚期CCS,对传统化疗耐药,于2012年1月开始使用舒尼替尼,37.5毫克/天,在疾病的原发和转移部位有放射学和代谢反应的证据。2012年4月切除的残留肿瘤显示出病理反应和Melan-A/MART-1抗原的缺失。在药物治疗期间对患者血液进行的免疫监测显示出全身性的、Melan-A/MART-1特异性免疫以及低频率的免疫抑制细胞。舒尼替尼于2012年5月重新开始使用,出现了新的反应,并持续了11个月,尽管由于毒性多次中断。每次治疗中断和重新开始时都记录了疾病进展和新的反应。2013年4月,由于疾病进展,舒尼替尼最终停药。
该病例分析证明,CCS表达的抗原与黑色素瘤一样,在体内可具有免疫原性,并且肿瘤抗原特异性T细胞可能在CCS患者中发挥抗肿瘤活性。因此,操纵免疫反应可能对这种STS亚型具有治疗潜力,免疫治疗方法可能是这些患者有前景的治疗选择。