Peasah Samuel K, Purakayastha Debjani Ram, Koul Parvaiz A, Dawood Fatima S, Saha Siddhartha, Amarchand Ritvik, Broor Shobha, Rastogi Vaibhab, Assad Romana, Kaul Kaisar Ahmed, Widdowson Marc-Alain, Lal Renu B, Krishnan Anand
College of Pharmacy, Mercer University, 3001 Mercer University Drive, Atlanta, GA, 30341-4155, USA.
Centers for Disease Control and Prevention, Atlanta, USA.
BMC Public Health. 2015 Apr 7;15:330. doi: 10.1186/s12889-015-1685-6.
Despite the high mortality and morbidity resulting from acute respiratory infections (ARI) globally, there are few data from low-income countries on costs of ARI to inform public health policy decisions We conducted a prospective survey to assess costs of ARI episodes in selected primary, secondary, and tertiary healthcare facilities in north India where no respiratory pathogen vaccine is routinely recommended.
Face-to-face interviews were conducted among a purposive sample of patients with ARI from healthcare facilities. Data were collected on out-of-pocket costs of hospitalization, medical consultations, medications, diagnostics, transportation, lodging, and missed work days. Telephone surveys were conducted two weeks after medical encounters to ask about subsequent missed work and costs incurred. Costs of prescriptions and diagnostics in public facilities were supplemented with WHO-CHOICE estimates of hospital bed costs. Missed work days were assigned cost based on the national annual per capita income (US$1,104). Non-medically attended ARI cases were identified from an ongoing community-based ARI surveillance project in Faridabad.
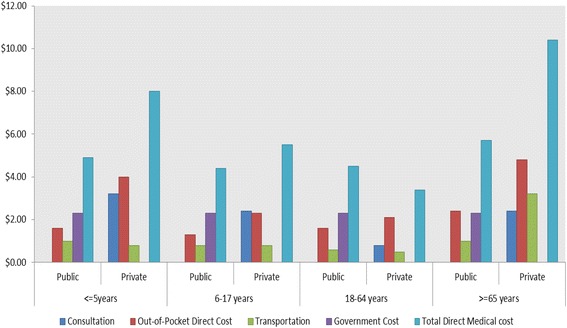
During September 2012-March 2013, 1766 patients with ARI were enrolled, including 451 hospitalized patients, 1056 outpatients, and 259 non-medically attended patients. The total direct cost of an ARI episode requiring outpatient care was US$4- $6 for public and $3-$10 for private institutions based on age groups. The total direct cost of an ARI episode requiring hospitalized care was $54-$120 in public and $135-$355 in private institutions. The cost of ARI among those hospitalized was highest among persons aged > = 65 years and lowest among children aged < 5 years. Indirect costs due to missed work days were 16-25% of total costs. The direct out-of-pocket cost of hospitalized ARI was 34% of annual per capita income.
The cost of hospitalized ARI episodes in India is high relative to median per capita income. Data from this study can inform evaluations of the cost effectiveness of proven ARI prevention strategies such as vaccination.
尽管全球急性呼吸道感染(ARI)导致的死亡率和发病率很高,但低收入国家关于ARI成本的数据很少,无法为公共卫生政策决策提供依据。我们开展了一项前瞻性调查,以评估印度北部部分未常规推荐呼吸道病原体疫苗的初级、二级和三级医疗机构中ARI发作的成本。
对来自医疗机构的ARI患者进行了有目的抽样的面对面访谈。收集了住院、医疗咨询、药物、诊断、交通、住宿和误工天数的自付费用数据。在医疗接触两周后进行电话调查,询问后续的误工情况和产生的费用。公共设施中处方和诊断的费用由世界卫生组织(WHO)-成本核算工具(CHOICE)对医院床位成本的估计进行补充。误工天数根据国家人均年收入(1104美元)估算成本。未就医的ARI病例是从法里达巴德正在进行的基于社区的ARI监测项目中识别出来的。
在2012年9月至2013年3月期间,共纳入1766例ARI患者,其中451例住院患者、1056例门诊患者和259例未就医患者。根据年龄组,需要门诊治疗的ARI发作的总直接成本在公共机构为4-6美元,在私立机构为3-10美元。需要住院治疗的ARI发作的总直接成本在公共机构为54-120美元,在私立机构为135-355美元。住院患者中ARI的成本在65岁及以上人群中最高,在5岁以下儿童中最低。误工天数导致的间接成本占总成本的16%-25%。住院ARI的直接自付费用占人均年收入的34%。
相对于人均收入中位数,印度住院ARI发作的成本较高。本研究的数据可为评估疫苗接种等已证实的ARI预防策略的成本效益提供参考。