Liu Peng, Bao Haidong, Zhang Xianbin, Zhang Jian, Ma Li, Wang Yulin, Li Chunyan, Wang Zhongyu, Gong Peng
Department of General Surgery, The First Affiliated Hospital of Dalian Medical University, 222 Zhongshan Road, 116011, Dalian, China.
Department of Epidemiology, Dalian Medical University, 9 Lvshun Road South, 116044, Dalian, China.
World J Surg Oncol. 2015 Feb 12;13:39. doi: 10.1186/s12957-015-0453-5.
Lithotomy (LT) and prone jackknife positions (PJ) are routinely used for abdominoperineal resection (APR). The present study compared the clinical, pathological, and oncological outcomes of PJ-APR vs. LT-APR in low rectal cancer patients in order to confirm which position will provide more benefits to patients undergoing APR.
This is a retrospective study of consecutive patients with low rectal cancer who underwent curative APR between January 2002 and December 2011. Patients were matched 1:2 (PJ-APR = 74 and LT-APR = 37 patients) based on gender and age. Perioperative data, postoperative outcomes, and survival were compared between the two approaches.
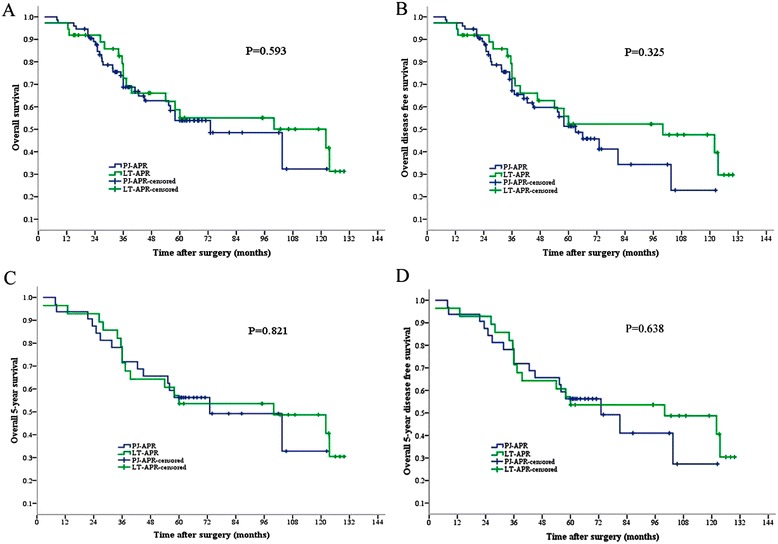
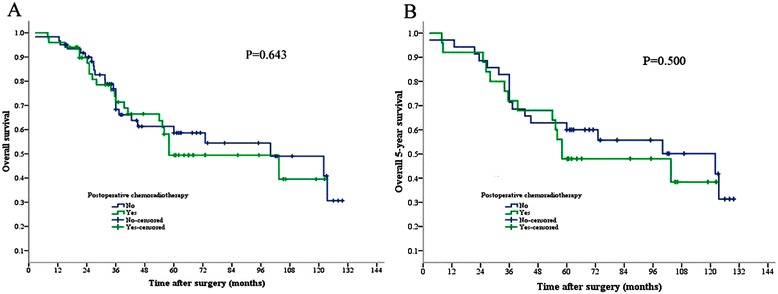
Hospital stay was shorter with PJ-APR compared with LT-APR (P < 0.05). Compared with LT-APR, duration of anesthesia (234 ± 50.8 vs. 291 ± 69 min, P = 0.022) and surgery (183 ± 44.8 vs. 234 ± 60 min, P = 0.016) was shorter with PJ-APR, and estimated blood losses were smaller (549 ± 218 vs. 674 ± 350 mL, P < 0.001). Blood transfusions were required in 37.8% of LT-APR patients and in 8.1% of PJ-APR patients (P < 0.001). There was no difference in the distribution of N stages (P = 0.27). Median follow-up was 47.1 (13.6-129.7) months. Postoperative complications were reported by fewer patients after PJ-APR compared with LT-APR (14.9% vs. 32.4%, P = 0.030). There were no significant differences in overall survival, disease-free survival, local recurrence, and distant metastasis (P > 0.05).
The PJ position provided a better exposure for low rectal cancer and had a lower operative risk and complication rates than LT-APR. However, there was no difference in rectal cancer prognosis between the two approaches. PJ-APR might be a better choice for patients with low rectal cancer.
截石位(LT)和俯卧折刀位(PJ)常用于腹会阴联合切除术(APR)。本研究比较了低位直肠癌患者行PJ-APR与LT-APR的临床、病理和肿瘤学结局,以确定哪种体位对接受APR的患者更有益。
这是一项对2002年1月至2011年12月期间接受根治性APR的连续低位直肠癌患者的回顾性研究。根据性别和年龄,患者按1:2匹配(PJ-APR组74例,LT-APR组37例)。比较两种手术方式的围手术期数据、术后结局和生存率。
与LT-APR相比,PJ-APR的住院时间更短(P<0.05)。与LT-APR相比,PJ-APR的麻醉时间(234±50.8 vs. 291±69分钟,P=0.022)和手术时间(183±44.8 vs. 234±60分钟,P=0.016)更短,估计失血量更少(549±218 vs. 674±350毫升,P<0.001)。LT-APR组37.8%的患者需要输血,PJ-APR组为8.1%(P<0.001)。N分期分布无差异(P=0.27)。中位随访时间为47.1(13.6-129.7)个月。与LT-APR相比,PJ-APR术后报告并发症的患者更少(14.9% vs. 32.4%,P=0.030)。总生存率、无病生存率、局部复发率和远处转移率无显著差异(P>0.05)。
PJ体位对低位直肠癌的暴露更好,手术风险和并发症发生率低于LT-APR。然而,两种手术方式在直肠癌预后方面无差异。PJ-APR可能是低位直肠癌患者的更好选择。