Flynn Darren, Nesbitt Daniel J, Ford Gary A, McMeekin Peter, Rodgers Helen, Price Christopher, Kray Christian, Thomson Richard G
Institute of Health and Society, Newcastle University, Baddiley-Clark Building, Richardson Road, Newcastle upon Tyne, UK.
School of Computing, Newcastle University, Newcastle upon Tyne, UK.
BMC Med Inform Decis Mak. 2015 Feb 7;15:6. doi: 10.1186/s12911-014-0127-1.
Thrombolytic treatment for acute ischaemic stroke improves prognosis, although there is a risk of bleeding complications leading to early death/severe disability. Benefit from thrombolysis is time dependent and treatment must be administered within 4.5 hours from onset of symptoms, which presents unique challenges for development of tools to support decision making and patient understanding about treatment. Our aim was to develop a decision aid to support patient-specific clinical decision-making about thrombolysis for acute ischaemic stroke, and clinical communication of personalised information on benefits/risks of thrombolysis by clinicians to patients/relatives.
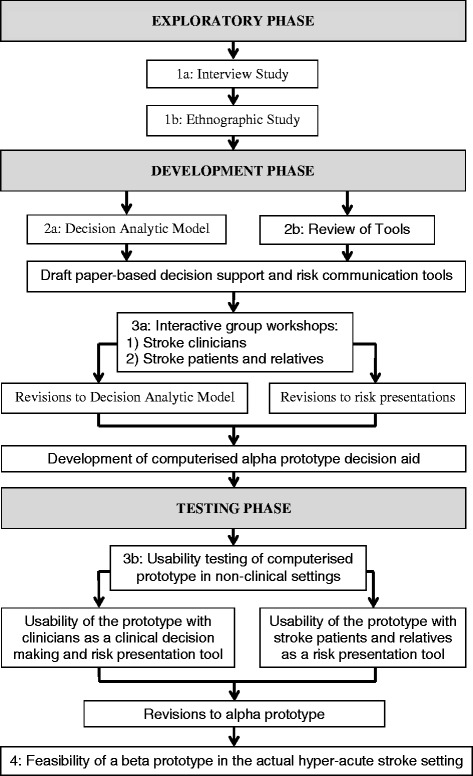
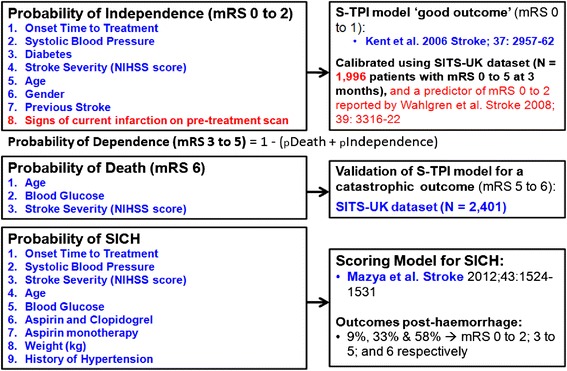
Using mixed methods we developed a COMPuterised decision Aid for Stroke thrombolysiS (COMPASS) in an iterative staged process (review of available tools; a decision analytic model; interactive group workshops with clinicians and patients/relatives; and prototype usability testing). We then tested the tool in simulated situations with final testing in real life stroke thrombolysis decisions in hospitals. Clinicians used COMPASS pragmatically in managing acute stroke patients potentially eligible for thrombolysis; their experience was assessed using self-completion forms and interviews. Computer logged data assessed time in use, and utilisation of graphical risk presentations and additional features. Patients'/relatives' experiences of discussions supported by COMPASS were explored using interviews.
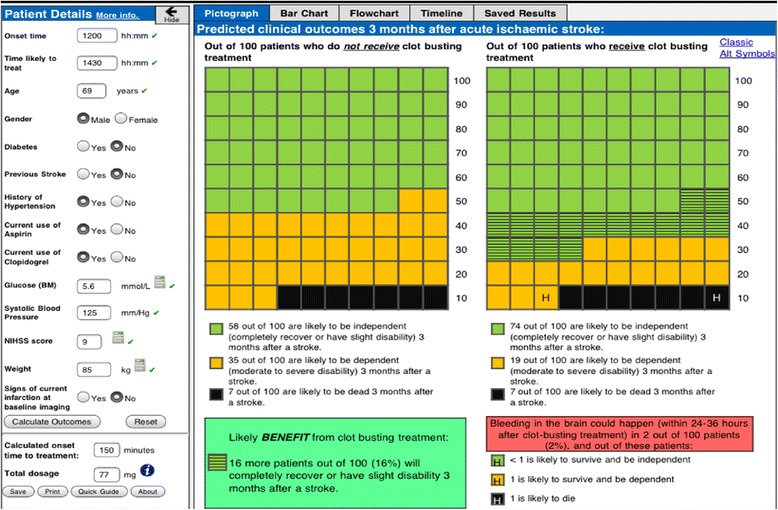
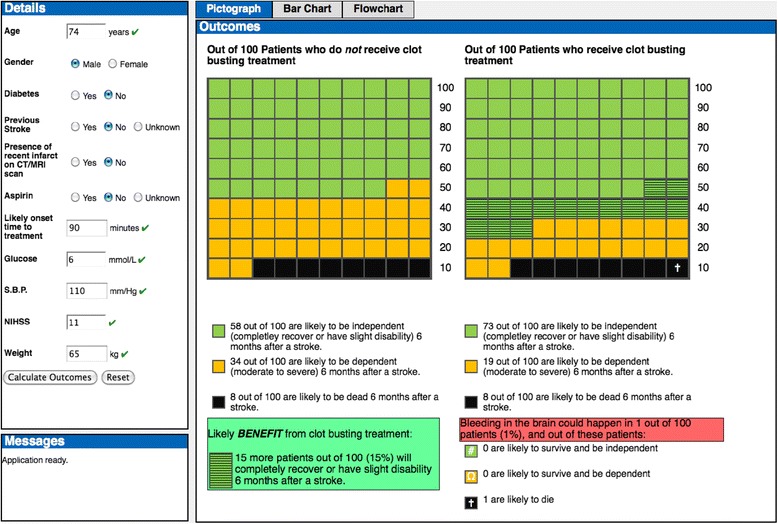
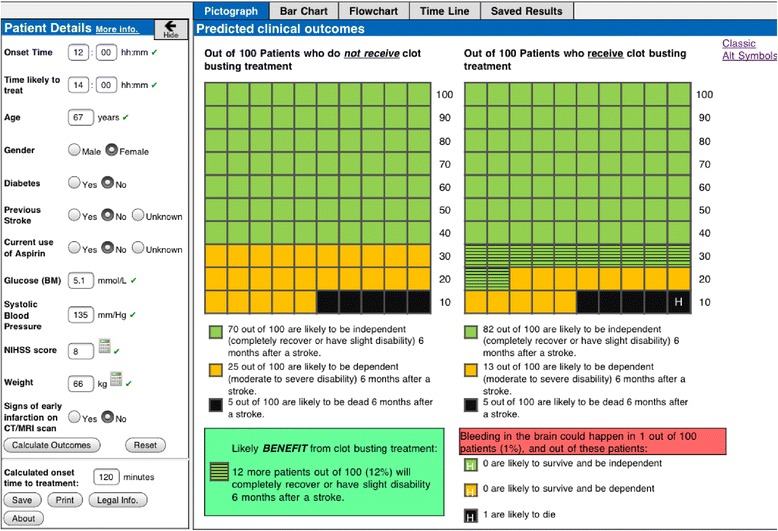
COMPASS expresses predicted outcomes (bleeding complications, death, and extent of disability) with and without thrombolysis, presented numerically (percentages and natural frequencies) and graphically (pictographs, bar graphs and flowcharts). COMPASS was used for 25 patients and no adverse effects of use were reported. Median time in use was 2.8 minutes. Graphical risk presentations were shared with 14 patients/relatives. Clinicians (n = 10) valued the patient-specific predictions of benefit from thrombolysis, and the support of better risk communication with patients/relatives. Patients (n = 2) and relatives (n = 6) reported that graphical risk presentations facilitated understanding of benefits/risks of thrombolysis. Additional features (e.g. dosage calculator) were suggested and subsequently embedded within COMPASS to enhance usability.
Our structured development process led to the development of a gamma prototype computerised decision aid. Initial evaluation has demonstrated reasonable acceptability of COMPASS amongst patients, relatives and clinicians. The impact of COMPASS on clinical outcomes requires wider prospective evaluation in clinical settings.
急性缺血性卒中的溶栓治疗可改善预后,尽管存在出血并发症导致早期死亡或严重残疾的风险。溶栓的益处具有时间依赖性,治疗必须在症状发作后4.5小时内进行,这为开发支持决策和帮助患者理解治疗的工具带来了独特挑战。我们的目标是开发一种决策辅助工具,以支持针对急性缺血性卒中溶栓的患者特异性临床决策,并支持临床医生向患者/亲属进行关于溶栓益处/风险的个性化信息的临床沟通。
我们采用混合方法,通过迭代分阶段过程(审查现有工具;建立决策分析模型;与临床医生及患者/亲属进行互动小组研讨会;以及原型可用性测试)开发了一种用于卒中溶栓的计算机化决策辅助工具(COMPASS)。然后我们在模拟情境中测试该工具,并在医院实际的卒中溶栓决策中进行最终测试。临床医生在管理可能适合溶栓的急性卒中患者时实际使用COMPASS;通过自我填写表格和访谈评估他们的体验。计算机记录数据评估使用时间、图形风险呈现的使用情况以及其他功能的使用情况。通过访谈探索患者/亲属在COMPASS支持下的讨论体验。
COMPASS以数字形式(百分比和自然频率)和图形形式(象形图、柱状图和流程图)呈现溶栓和不溶栓的预测结果(出血并发症、死亡和残疾程度)。COMPASS用于25例患者,未报告使用不良反应。中位使用时间为2.8分钟。向14例患者/亲属展示了图形风险呈现。临床医生(n = 10)重视COMPASS对溶栓益处的患者特异性预测,以及对与患者/亲属进行更好的风险沟通的支持。患者(n = 2)和亲属(n = 6)报告称,图形风险呈现有助于理解溶栓的益处/风险。有人提出了其他功能(如剂量计算器),随后将其嵌入COMPASS以提高可用性。
我们的结构化开发过程促成了伽马原型计算机化决策辅助工具的开发。初步评估表明COMPASS在患者、亲属和临床医生中具有合理的可接受性。COMPASS对临床结局的影响需要在临床环境中进行更广泛的前瞻性评估。