Duke Clinical Research Institute, Durham, NC, USA; Division of Pulmonary, Allergy and Critical Care Medicine, Department of Medicine, Duke University, Durham, NC, USA.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, University of California, San Francisco, CA, USA.
Lancet Respir Med. 2015 May;3(5):388-96. doi: 10.1016/S2213-2600(15)00093-4. Epub 2015 Apr 15.
Mortality is an impractical primary endpoint for clinical trials in patients with idiopathic pulmonary fibrosis who have mild-to-moderate physiological impairment because event rates are low. Change in forced vital capacity (FVC) is widely accepted as a surrogate for mortality and is the most common primary endpoint in clinical trials for this disorder. Use of hospital admission as a predictor for mortality, independent of FVC decline, has not been well defined. We aimed to ascertain the independent and combined association of hospital admission and at least a 10% decrease in FVC with all-cause mortality.
We did a pooled cohort study of 517 patients with idiopathic pulmonary fibrosis from three IPFnet multicentre randomised controlled trials. We compared the incidence of non-elective hospital admission and a 10% or greater reduction in FVC across strata of baseline physiological impairment. We used Cox proportional-hazards models to assess the risk of all-cause mortality associated with these surrogate events, occurring up to a predefined landmark timepoint. The three studies are registered at ClinicalTrials.gov, numbers NCT00650091, NCT00517933, and NCT00957242.
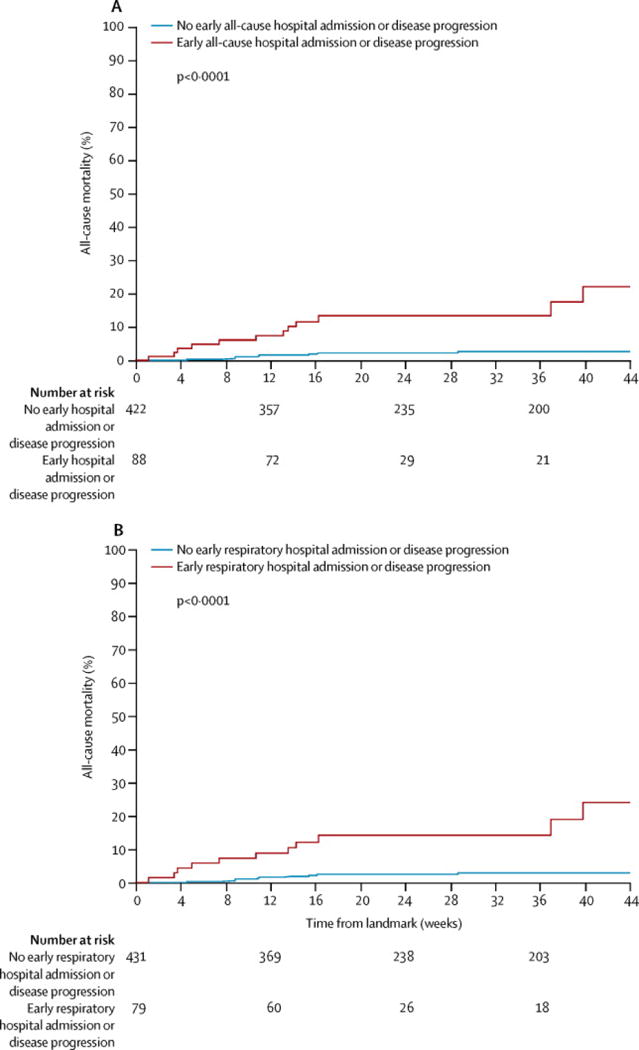
Seven patients died before the landmark timepoint. Of the 510 patients remaining, 38 (7%) were admitted to hospital up to the predefined timepoint and 58 (11%) had a categorical decrease in FVC of at least 10%. Most patients admitted to hospital did not have a 10% or greater decrease in FVC (30 vs eight). Both surrogate events were associated with subsequent time to death from any cause (hazard ratio [HR] for admission 4·05, 95% CI 1·36-12·11 vs HR for 10% or greater decline in FVC 4·68, 1·83-11·99). When causes of hospital admission were considered, only respiratory events were associated with mortality (5·97, 1·81-19·74).
Hospital admission might be an appropriate component of a clinically meaningful composite endpoint that improves the feasibility of clinical trials in idiopathic pulmonary fibrosis. Further studies are needed to refine the most appropriate definition of hospital admission for future trials.
US National Heart, Lung, and Blood Institute (NHLBI), and The Cowlin Family Fund at the Chicago Community Trust.
对于患有特发性肺纤维化且存在轻至中度生理损伤的患者,死亡率是临床试验中不切实际的主要终点,因为事件发生率较低。用力肺活量(FVC)的变化被广泛认为是死亡率的替代指标,也是该疾病临床试验中最常见的主要终点。尚未明确将住院作为独立于 FVC 下降的死亡率预测因素的使用情况。我们旨在确定住院和 FVC 至少下降 10%与全因死亡率的独立和联合关联。
我们对来自三个 IPFnet 多中心随机对照试验的 517 名特发性肺纤维化患者进行了汇总队列研究。我们比较了基线生理损伤不同分层中无择期住院和 FVC 下降 10%或更多的发生率。我们使用 Cox 比例风险模型评估这些替代事件发生时与全因死亡率相关的风险,这些事件一直发生到预定的时间点。这三项研究均在 ClinicalTrials.gov 注册,编号分别为 NCT00650091、NCT00517933 和 NCT00957242。
7 名患者在预定时间点前死亡。在剩余的 510 名患者中,38 名(7%)在预定时间点前住院,58 名(11%)FVC 出现至少 10%的分类下降。大多数住院患者没有 FVC 下降 10%或更多(30 名比 8 名)。两个替代事件均与随后的全因死亡时间相关(住院的危险比[HR]为 4.05,95%CI 为 1.36-12.11 与 FVC 下降 10%或更多的 HR 为 4.68,1.83-11.99)。当考虑住院的原因时,只有呼吸事件与死亡率相关(5.97,1.81-19.74)。
住院可能是特发性肺纤维化临床试验中更可行的有意义的综合终点的一个组成部分。需要进一步的研究来完善未来试验中最适合的住院定义。
美国国立心肺血液研究所(NHLBI)和芝加哥社区信托公司的 Cowlin 家族基金。