Nguyen Paul L, Jarolim Petr, Basaria Shehzad, Zuflacht Jonah P, Milian Jessica, Kadivar Samoneh, Graham Powell L, Hyatt Andrew, Kantoff Philip W, Beckman Joshua A
Radiation Oncology, Brigham and Women's Hospital and Dana-Farber Cancer Institute, Boston, MA (P.L.N., P.L.G., A.H.).
Department of Pathology, Brigham and Women's Hospital, Boston, MA (P.J.).
J Am Heart Assoc. 2015 Apr 20;4(4):e001914. doi: 10.1161/JAHA.115.001914.
Androgen deprivation therapy (ADT) is a standard treatment for patients with aggressive prostate cancer. Although ADT improves survival, it increases the risk of diabetes. Emerging evidence suggests that ADT increases adverse cardiovascular events as early as 3 months after initiation in patients with cardiovascular disease, but the mechanism is unknown. We hypothesized that ADT may impair endothelium-dependent vasodilation due to increases in lipids and insulin resistance and may provide a link for heightened cardiovascular risk in this population.
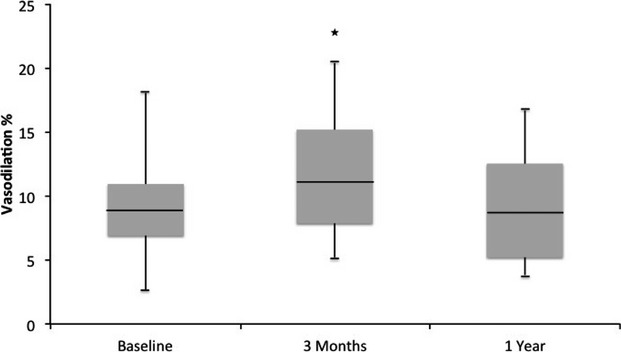
We prospectively evaluated conduit artery endothelium-dependent and -independent vasodilation, lipids, and insulin resistance in 16 consecutively treated men (mean age 66 ± 7 years; 25% with diabetes) with prostate cancer before and after 3 months of ADT. High-resolution B-mode ultrasound was used to assess flow-mediated (endothelium-dependent) and nitroglycerine-mediated (endothelium-independent) brachial artery vasodilation. ADT significantly increased insulin resistance, total cholesterol, HDL, and LDL. Endothelium-dependent vasodilation was greater at 3 months than at baseline (10.8% [interquartile range: 7.7% to 14.6%] versus 8.9% [interquartile range: 4.0% to 12.6%], respectively; P=0.046, allometric P=0.037). Nitroglycerine-mediated vasodilation did not change from baseline (P>0.2). The subset of participants on ADT for 6 months returned for reevaluation at 1 year. In this group, endothelium-dependent vasodilation increased from baseline to 3 months and returned to baseline 6 months after ADT withdrawal (9.4% [interquartile range: 6.9% to 10.9%], 11.6% [interquartile range: 7.9% to 15.2%], and 9.0% [interquartile range: 5.1% to 12.5%], respectively; P=0.05).
In contrast to our expectation, ADT improved endothelium-dependent vasodilation and its cessation returned endothelium-dependent vasodilation to baseline. Determining the mechanism of this change requires further investigation.
雄激素剥夺疗法(ADT)是侵袭性前列腺癌患者的标准治疗方法。尽管ADT可提高生存率,但会增加患糖尿病的风险。新出现的证据表明,ADT在心血管疾病患者开始治疗后3个月就会增加不良心血管事件的风险,但其机制尚不清楚。我们推测,ADT可能由于脂质增加和胰岛素抵抗而损害内皮依赖性血管舒张,并可能为该人群心血管风险升高提供一个联系。
我们前瞻性评估了16例连续接受治疗的前列腺癌男性患者(平均年龄66±7岁;25%患有糖尿病)在ADT治疗3个月前后的导管动脉内皮依赖性和非内皮依赖性血管舒张、脂质和胰岛素抵抗情况。使用高分辨率B型超声评估血流介导的(内皮依赖性)和硝酸甘油介导的(非内皮依赖性)肱动脉血管舒张。ADT显著增加了胰岛素抵抗、总胆固醇、高密度脂蛋白和低密度脂蛋白。3个月时内皮依赖性血管舒张大于基线时(分别为10.8%[四分位间距:7.7%至14.6%]对8.9%[四分位间距:4.0%至12.6%];P=0.046,异速生长P=0.037)。硝酸甘油介导的血管舒张与基线相比没有变化(P>0.2)。接受ADT治疗6个月的参与者子集在1年时返回进行重新评估。在该组中,内皮依赖性血管舒张从基线增加到3个月,并在ADT停药6个月后恢复到基线(分别为9.4%[四分位间距:6.9%至10.9%]、11.6%[四分位间距:7.9%至15.2%]和9.0%[四分位间距:5.1%至12.5%];P=0.05)。
与我们的预期相反,ADT改善了内皮依赖性血管舒张,其停止后内皮依赖性血管舒张恢复到基线水平。确定这种变化的机制需要进一步研究。