Speer Timo, Groesdonk Heinrich V, Zapf Beate, Buescher Vanessa, Beyse Miriam, Duerr Laura, Gewert Stella, Krauss Patrizia, Poppleton Aaron, Wagenpfeil Stefan, Fliser Danilo, Schaefers Hans-Joachim, Klingele Matthias
Department of Internal Medicine, Nephrology and Hypertension, Saarland University Medical Centre, Kirrberger Strasse, D-66424, Homburg/Saar, Germany.
Department of Thoracic and Cardiovascular Surgery, Saarland University Medical Centre, Homburg/Saar, Germany.
Crit Care. 2015 Apr 23;19(1):190. doi: 10.1186/s13054-015-0925-6.
Several scoring systems have been developed to predict postoperative mortality and complications in patients undergoing cardiac surgery. However, these computer-based calculations are time- and cost-intensive. A simple but highly predictive test for postoperative risk would be of clinical benefit with respect to increasingly scarce hospital resources. We therefore assessed the predictive power of fibroblast growth factor 23 (FGF23) measurement compared with an established scoring system.
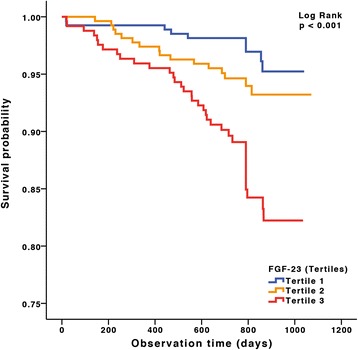
We conducted a prospective interdisciplinary observational study at the Saarland University Medical Centre that included 859 patients undergoing elective cardiac surgery between January 2010 and March 2011 with a median follow-up after discharge of 822 days. We compared a single preoperative measurement of FGF23 as a prognostic tool with the 18 parameters comprising EuroSCORE II with respect to postoperative mortality, acute kidney injury, non-occlusive mesenteric ischemia, clinical course and long-term outcome.
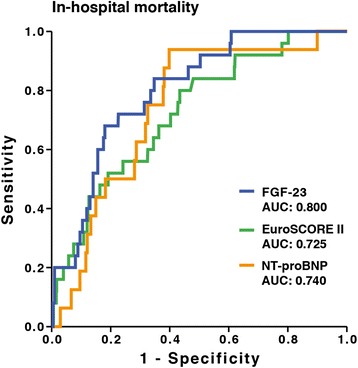
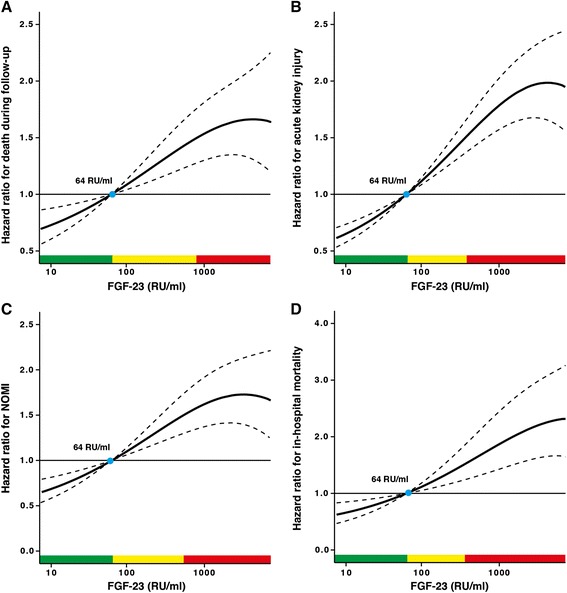
Preoperative FGF23 levels were highly predictive of postoperative outcome and complications. The predictive value of FGF23 for mortality in the receiver operating characteristic curve was greater than the EuroSCORE II (area under the curve: 0.800 versus 0.725). Moreover, preoperative FGF23 independently predicted postoperative acute kidney injury and non-occlusive mesenteric ischemia comparably to the EuroSCORE II. Finally, FGF23 was found to be an independent predictor of clinical course parameters, including duration of surgery, ventilation time and length of stay.
In patients undergoing elective cardiac surgery, a simple preoperative FGF23 measurement is a powerful indicator of surgical mortality, postoperative complications and long-term outcome. Its utility compares to the widely used EuroSCORE II.
已经开发了几种评分系统来预测心脏手术患者的术后死亡率和并发症。然而,这些基于计算机的计算既耗时又成本高昂。对于日益稀缺的医院资源而言,一种简单但具有高度预测性的术后风险测试将具有临床益处。因此,我们评估了与既定评分系统相比,成纤维细胞生长因子23(FGF23)测量的预测能力。
我们在萨尔州大学医学中心进行了一项前瞻性跨学科观察性研究,纳入了2010年1月至2011年3月期间接受择期心脏手术的859例患者,出院后中位随访时间为822天。我们将术前单次FGF23测量作为一种预后工具,与包含欧洲心脏手术风险评估系统(EuroSCORE)II的18个参数进行比较,以评估术后死亡率、急性肾损伤、非闭塞性肠系膜缺血、临床病程和长期结局。
术前FGF23水平对术后结局和并发症具有高度预测性。在受试者工作特征曲线中,FGF23对死亡率的预测价值大于EuroSCORE II(曲线下面积:0.800对0.725)。此外,术前FGF23与EuroSCORE II相当,独立预测术后急性肾损伤和非闭塞性肠系膜缺血。最后,发现FGF23是临床病程参数的独立预测因子,包括手术时间、通气时间和住院时间。
在接受择期心脏手术的患者中,术前简单的FGF23测量是手术死亡率、术后并发症和长期结局的有力指标。其效用与广泛使用的EuroSCORE II相当。