Cea Soriano Lucia, Johansson Saga, Stefansson Bergur, Rodríguez Luis A García
Spanish Centre for Pharmacoepidemiologic Research (CEIFE), Almirante 28-2, E 28004, Madrid, Spain.
AstraZeneca R&D, Mölndal, Sweden.
Cardiovasc Diabetol. 2015 Apr 18;14:38. doi: 10.1186/s12933-015-0204-5.
Diabetes and chronic kidney disease (CKD) are independent predictors of death and cardiovascular events and their concomitant prevalence has increased in recent years. The aim of this study was to characterize the effect of the estimated glomerular filtration rate (eGFR) and other factors on the risk of death and cardiovascular events in patients with type 2 diabetes.
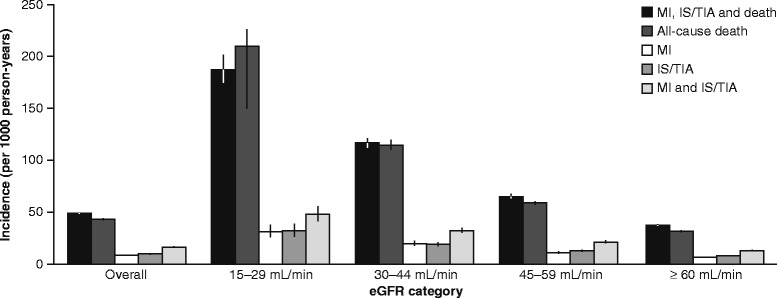
A cohort of 57,946 patients with type 2 diabetes who were aged 20-89 years in 2000-2005 was identified from The Health Improvement Network, a UK primary care database. Incidence rates of death, myocardial infarction (MI), and ischemic stroke or transient ischemic attack (IS/TIA) were calculated overall and by eGFR category at baseline. eGFR was calculated using the Modification of Diet in Renal Disease (MDRD) study equation. Death, MI and IS/TIA cases were detected using an automatic computer search and IS/TIA cases were further ascertained by manual review of medical records. Hazard ratios (HRs) and their corresponding 95% confidence intervals (CIs) for death, MI, and IS/TIA associated with eGFR category and other factors were estimated using Cox regression models adjusted for potential confounders.
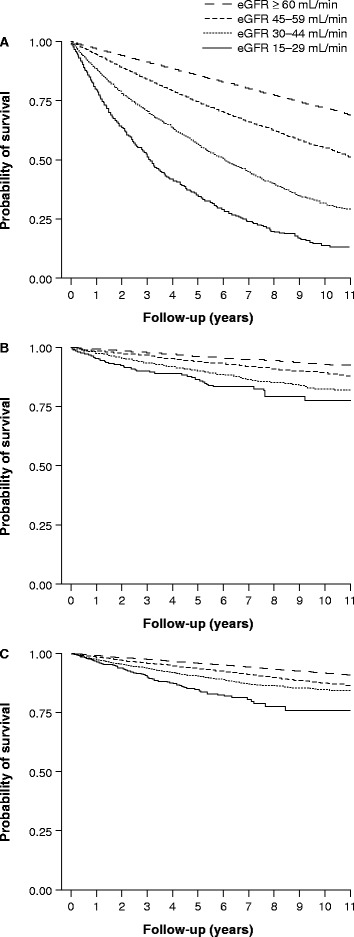
Overall incidence rates of death (mean follow-up time of 6.76 years), MI (6.64 years) and IS/TIA (6.56 years) were 43.65, 9.26 and 10.39 cases per 1000 person-years, respectively. A low eGFR (15-29 mL/min) was associated with an increased risk of death (HR: 2.79; 95% CI: 2.57-3.03), MI (HR: 2.33; 95% CI: 1.89-2.87) and IS/TIA (HR: 1.77; 95% CI: 1.43-2.18) relative to eGFR ≥ 60 mL/min. Other predictors of death, MI and IS/TIA included age, longer duration of diabetes, poor control of diabetes, hyperlipidemia, smoking and a history of cardiovascular events.
In patients with type 2 diabetes, management of cardiovascular risk factors and careful monitoring of eGFR may represent opportunities to reduce the risks of death, MI and IS/TIA.
糖尿病和慢性肾脏病(CKD)是死亡和心血管事件的独立预测因素,近年来它们的合并患病率有所上升。本研究的目的是描述估计肾小球滤过率(eGFR)及其他因素对2型糖尿病患者死亡和心血管事件风险的影响。
从英国初级保健数据库“健康改善网络”中识别出一组在2000 - 2005年年龄为20 - 89岁的57946例2型糖尿病患者。计算总体以及基线时按eGFR类别划分的死亡、心肌梗死(MI)、缺血性卒中或短暂性脑缺血发作(IS/TIA)的发病率。eGFR使用肾脏病饮食改良(MDRD)研究方程计算。通过自动计算机搜索检测死亡、MI和IS/TIA病例,并通过人工查阅病历进一步确定IS/TIA病例。使用针对潜在混杂因素进行调整的Cox回归模型估计与eGFR类别及其他因素相关的死亡、MI和IS/TIA的风险比(HRs)及其相应的95%置信区间(CIs)。
死亡(平均随访时间6.76年)、MI(6.64年)和IS/TIA(6.56年)的总体发病率分别为每1000人年43.65例、9.26例和10.39例。与eGFR≥60 mL/min相比,低eGFR(15 - 29 mL/min)与死亡风险增加(HR:2.79;95% CI:2.57 - 3.03)、MI风险增加(HR:2.33;95% CI:1.89 - 2.87)和IS/TIA风险增加(HR:1.77;95% CI:1.43 - 2.18)相关。死亡、MI和IS/TIA的其他预测因素包括年龄、糖尿病病程较长、糖尿病控制不佳、高脂血症、吸烟和心血管事件史。
在2型糖尿病患者中,管理心血管危险因素并仔细监测eGFR可能是降低死亡、MI和IS/TIA风险 的机会。