Ker Katharine, Tansley Gavin, Beecher Deirdre, Perner Anders, Shakur Haleema, Harris Tim, Roberts Ian
Cochrane Injuries Group, London School of Hygiene & TropicalMedicine, Room 186, Keppel Street, London, WC1E 7HT, UK.
Cochrane Database Syst Rev. 2015 Feb 26;2015(2):CD011386. doi: 10.1002/14651858.CD011386.pub2.
Dehydration is an important cause of death in patients with Ebola virus disease (EVD). Parenteral fluids are often required in patients with fluid requirements in excess of their oral intake. The peripheral intravenous route is the most commonly used method of parenteral access, but inserting and maintaining an intravenous line can be challenging in the context of EVD. Therefore it is important to consider the advantages and disadvantages of different routes for achieving parenteral access (e.g. intravenous, intraosseous, subcutaneous and intraperitoneal).
To compare the reliability, ease of use and speed of insertion of different parenteral access methods.
We ran the search on 17 November 2014. We searched the Cochrane Injuries Group's Specialised Register, Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library), Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE(R) and Ovid OLDMEDLINE(R), Embase Classic + Embase (OvidSP), CINAHL (EBSCOhost), clinicaltrials.gov and screened reference lists.
Randomised controlled trials comparing different parenteral routes for the infusion of fluids or medication.
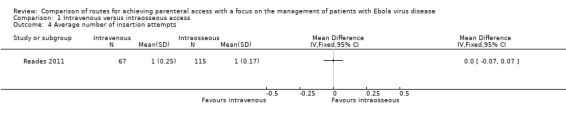
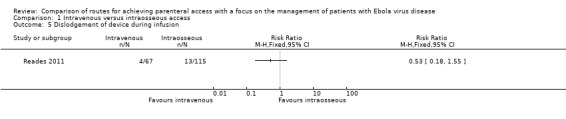
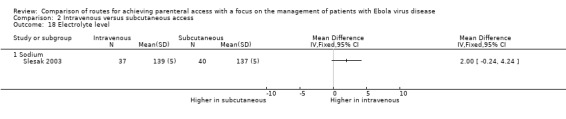
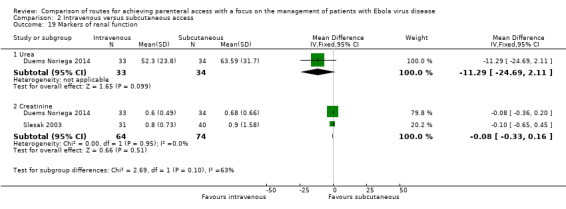
Two review authors examined the titles and abstracts of records obtained by searching the electronic databases to determine eligibility. Two review authors extracted data from the included trials and assessed the risk of bias. Outcome measures of interest were success of insertion; time required for insertion; number of insertion attempts; number of dislodgements; time period with functional access; local site reactions; clinicians' perception of ease of administration; needlestick injury to healthcare workers; patients' discomfort; and mortality. For trials involving the administration of fluids we also collected data on the volume of fluid infused, changes in serum electrolytes and markers of renal function. We rated the quality of the evidence as 'high', 'moderate', 'low' or 'very low' according to the GRADE approach for the following outcomes: success of insertion, time required for insertion, number of dislodgements, volume of fluid infused and needlestick injuries.
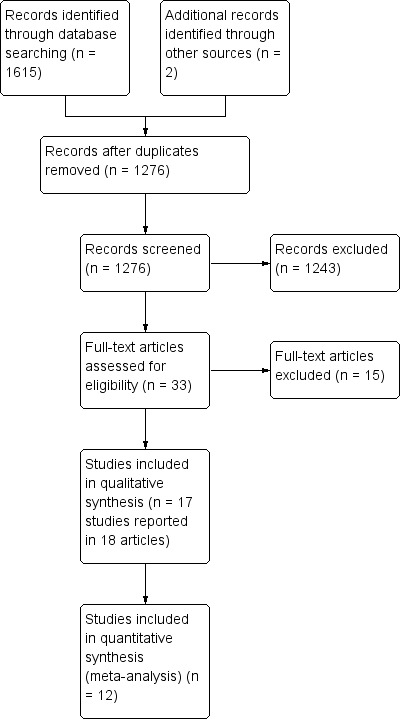
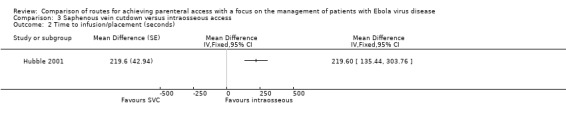
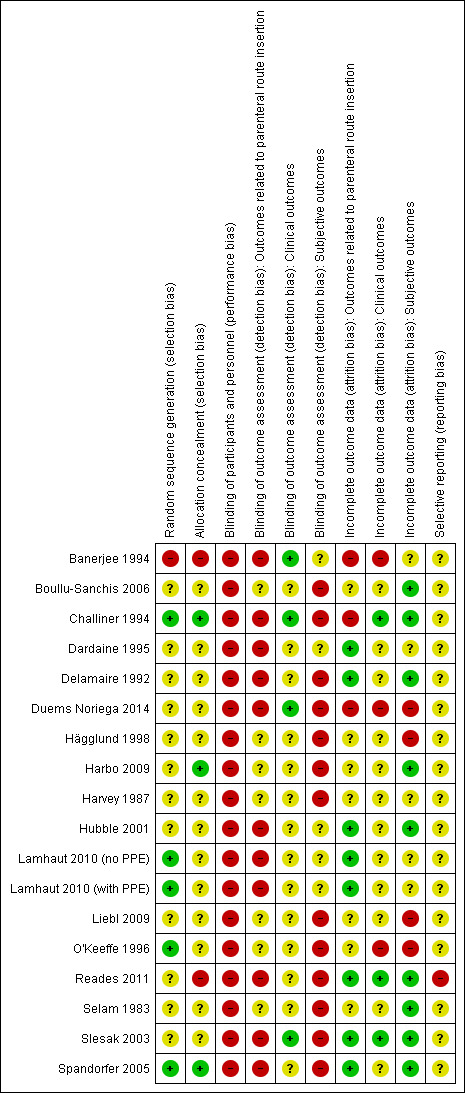
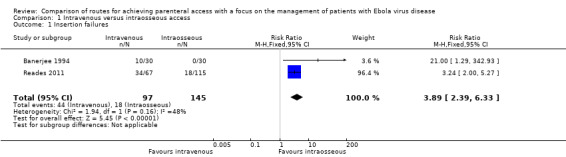
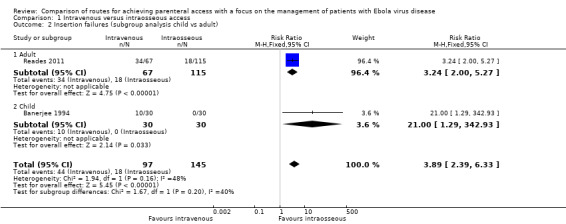
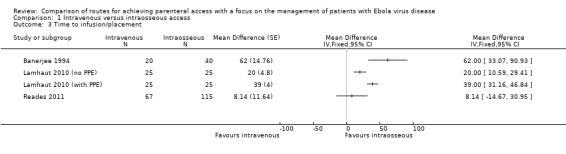
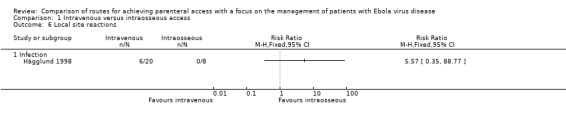
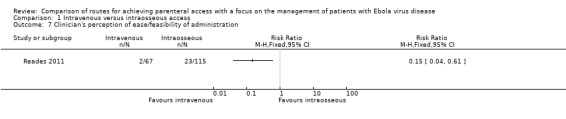
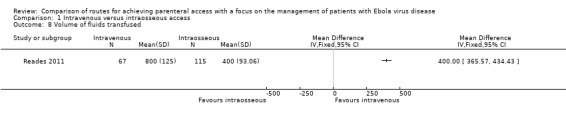
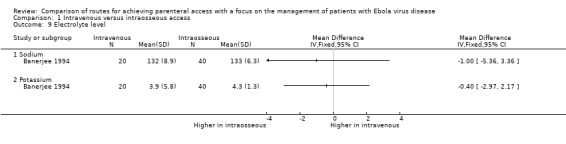
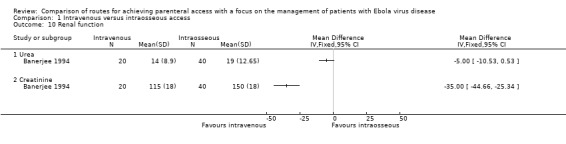
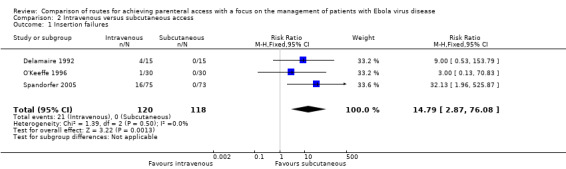
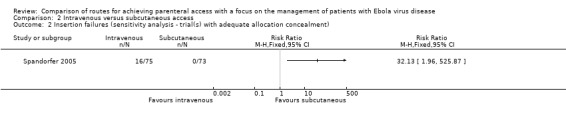
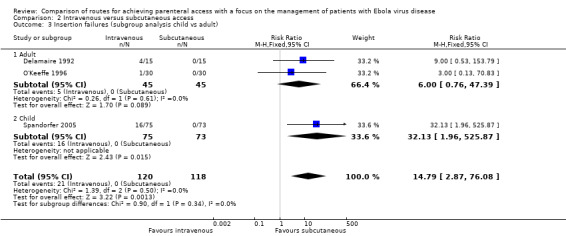
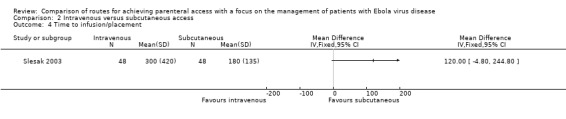
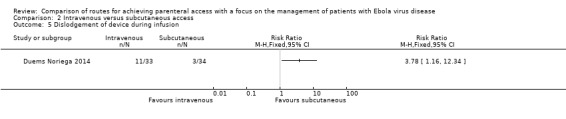
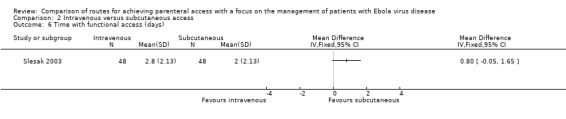
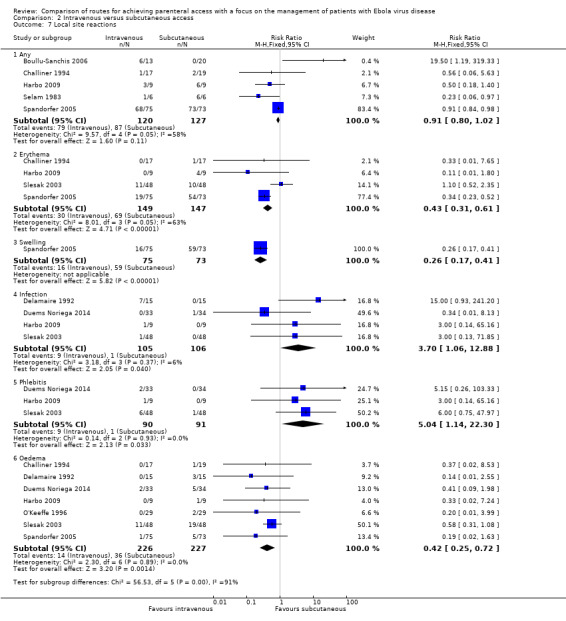
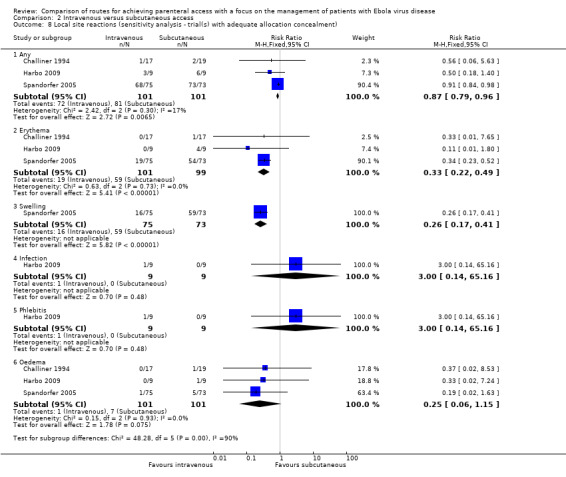
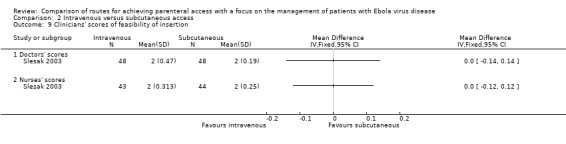
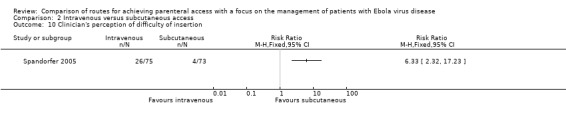
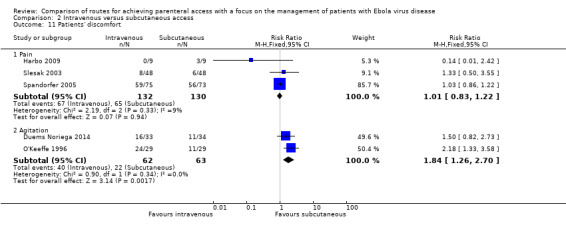
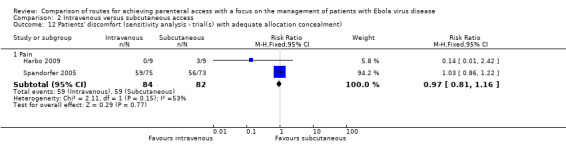
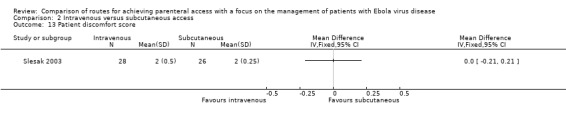
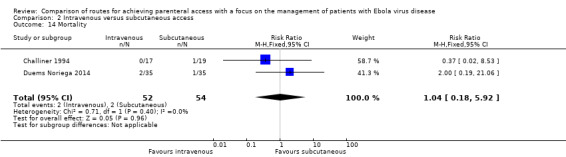
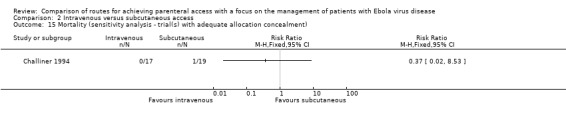
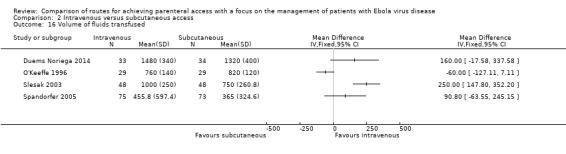
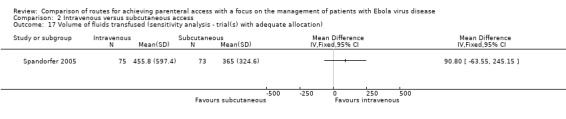
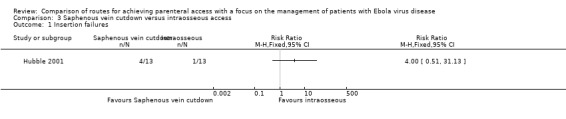
We included 17 trials involving 885 participants. Parenteral access was used to infuse fluids in 11 trials and medications in six trials. None of the trials involved patients with EVD. Intravenous and intraosseous access was compared in four trials; intravenous and subcutaneous access in 11; peripheral intravenous and intraperitoneal access in one; saphenous vein cutdown and intraosseous access in one; and intraperitoneal with subcutaneous access in one. All of the trials assessing the intravenous method involved peripheral intravenous access.We judged few trials to be at low risk of bias for any of the assessed domains.Compared to the intraosseous group, patients in the intravenous group were more likely to experience an insertion failure (risk ratio (RR) 3.89, 95% confidence interval (CI) 2.39 to 6.33; n = 242; GRADE rating: low). We did not pool data for time to insertion but estimates from the trials suggest that inserting intravenous access takes longer (GRADE rating: moderate). Clinicians judged the intravenous route to be easier to insert (RR 0.15, 95% CI 0.04 to 0.61; n = 182). A larger volume of fluids was infused via the intravenous route (GRADE rating: moderate). There was no evidence of a difference between the two routes for any other outcomes, including adverse events.Compared to the subcutaneous group, patients in the intravenous group were more likely to experience an insertion failure (RR 14.79, 95% CI 2.87 to 76.08; n = 238; GRADE rating: moderate) and dislodgement of the device (RR 3.78, 95% CI 1.16 to 12.34; n = 67; GRADE rating: low). Clinicians also judged the intravenous route as being more difficult to insert and patients were more likely to be agitated in the intravenous group. Patients in the intravenous group were more likely to develop a local infection and phlebitis, but were less likely to develop erythema, oedema or swelling than those in the subcutaneous group. A larger volume of fluids was infused into patients via the intravenous route. There was no evidence of a difference between the two routes for any other outcome.There were insufficient data to reliably determine if the risk of insertion failure differed between the saphenous vein cutdown (SVC) and intraosseous method (RR 4.00, 95% CI 0.51 to 31.13; GRADE rating: low). Insertion using SVC took longer than the intraosseous method (MD 219.60 seconds, 95% CI 135.44 to 303.76; GRADE rating: moderate). There were no data and therefore there was no evidence of a difference between the two routes for any other outcome.There were insufficient data to reliably determine the relative effects of intraperitoneal or central intravenous access relative to any other parenteral access method.
AUTHORS' CONCLUSIONS: There are several different ways of achieving parenteral access in patients who are unable meet their fluid requirements with oral intake alone. The quality of the evidence, as assessed using the GRADE criteria, is somewhat limited because of the lack of adequately powered trials at low risk of bias. However, we believe that there is sufficient evidence to draw the following conclusions: if peripheral intravenous access can be achieved easily, this allows infusion of larger volumes of fluid than other routes; but if this is not possible, the intraosseous and subcutaneous routes are viable alternatives. The subcutaneous route may be suitable for patients who are not severely dehydrated but in whom ongoing fluid losses cannot be met by oral intake.A film to accompany this review can be viewed here (http://youtu.be/ArVPzkf93ng).
脱水是埃博拉病毒病(EVD)患者死亡的重要原因。对于液体需求超过经口摄入量的患者,通常需要胃肠外补液。外周静脉途径是最常用的胃肠外补液通路,但在埃博拉病毒病的情况下,插入并维持静脉通路可能具有挑战性。因此,考虑不同途径实现胃肠外补液通路(如静脉、骨内、皮下和腹腔内)的优缺点很重要。
比较不同胃肠外补液通路方法的可靠性、易用性和插入速度。
我们于2014年11月17日进行检索。我们检索了Cochrane损伤组专业注册库、Cochrane对照试验中心注册库(CENTRAL,Cochrane图书馆)、Ovid MEDLINE(R)在研及其他非索引引文、Ovid MEDLINE(R)每日更新、Ovid MEDLINE(R)和Ovid OLDMEDLINE(R)、Embase经典版+Embase(OvidSP)、CINAHL(EBSCOhost)、clinicaltrials.gov,并筛选了参考文献列表。
比较不同胃肠外补液途径输注液体或药物的随机对照试验。
两位综述作者检查了通过检索电子数据库获得的记录的标题和摘要,以确定其是否符合纳入标准。两位综述作者从纳入的试验中提取数据,并评估偏倚风险。感兴趣的结局指标包括:插入成功;插入所需时间;插入尝试次数;移位次数;功能通路的时间段;局部部位反应;临床医生对给药 ease 的感知;医护人员针刺伤;患者不适;以及死亡率。对于涉及液体输注的试验,我们还收集了输注液体量、血清电解质变化和肾功能指标的数据。根据GRADE方法,我们将以下结局的证据质量评为“高”、“中”、“低”或“极低”:插入成功、插入所需时间、移位次数、输注液体量和针刺伤。
我们纳入了17项试验,涉及885名参与者。11项试验使用胃肠外补液通路输注液体,6项试验输注药物。所有试验均未涉及埃博拉病毒病患者。四项试验比较了静脉和骨内通路;11项试验比较了静脉和皮下通路;一项试验比较了外周静脉和腹腔内通路;一项试验比较了大隐静脉切开术和骨内通路;一项试验比较了腹腔内和皮下通路。所有评估静脉方法的试验均涉及外周静脉通路。我们认为几乎没有试验在任何评估领域的偏倚风险较低。与骨内组相比,静脉组患者更有可能插入失败(风险比(RR)3.89,95%置信区间(CI)2.39至6.33;n = 242;GRADE评级:低)。我们未汇总插入时间的数据,但试验估计表明插入静脉通路所需时间更长(GRADE评级:中)。临床医生认为静脉途径更容易插入(RR 0.15,95%CI 0.04至0.61;n = 182)。通过静脉途径输注的液体量更大(GRADE评级:中)。对于任何其他结局,包括不良事件,没有证据表明两种途径之间存在差异。与皮下组相比,静脉组患者更有可能插入失败(RR 14.79,95%CI 2.87至76.08;n = 238;GRADE评级:中)和装置移位(RR 3.78,95%CI 1.16至12.34;n = 67;GRADE评级:低)。临床医生也认为静脉途径更难插入,并且静脉组患者更有可能烦躁不安。静脉组患者更有可能发生局部感染和静脉炎,但与皮下组相比,发生红斑、水肿或肿胀的可能性较小。通过静脉途径向患者输注的液体量更大。对于任何其他结局,没有证据表明两种途径之间存在差异。没有足够的数据来可靠地确定大隐静脉切开术(SVC)和骨内方法之间插入失败的风险是否存在差异(RR 4.00,95%CI 0.51至31.13;GRADE评级:低)。使用SVC插入比骨内方法花费的时间更长(MD 219.60秒,95%CI 135.44至303.76;GRADE评级:中)。没有数据,因此对于任何其他结局,没有证据表明两种途径之间存在差异。没有足够的数据来可靠地确定腹腔内或中心静脉通路相对于任何其他胃肠外补液通路方法的相对效果。
对于仅通过口服摄入无法满足液体需求的患者,有几种不同的实现胃肠外补液通路的方法。由于缺乏足够样本量且偏倚风险低的试验,使用GRADE标准评估的证据质量在一定程度上受到限制。然而,我们认为有足够的证据得出以下结论:如果能够轻松实现外周静脉通路,这允许比其他途径输注更大体积的液体;但如果无法实现,骨内和皮下途径是可行的替代方法。皮下途径可能适用于未严重脱水但经口摄入无法满足持续液体丢失的患者。可在此处观看与本综述相关的影片(http://youtu.be/ArVPzkf93ng)。