Yousaf Nadia, Harris Samuel, Martin-Liberal Juan, Stanway Susannah, Linch Mark, Ifijen Maria, Al Muderis Omar, Khabra Komel, Fisher Cyril, Noujaim Jonathan, Judson Ian, Benson Charlotte
The Sarcoma Unit, The Royal Marsden Hospital, Fulham Road, London, SW3 6JJ UK.
Clin Sarcoma Res. 2015 Mar 24;5:10. doi: 10.1186/s13569-015-0026-y. eCollection 2015.
The efficacy and toxicity of first line palliative chemotherapy for soft tissue sarcomas (STS) in the elderly is poorly described.
Patients over the age of 65 years receiving first line chemotherapy for advanced non-GIST STS January 1998 - January 2012 at the Royal Marsden Hospital were identified. Data regarding survival and predictive factors were collected retrospectively.
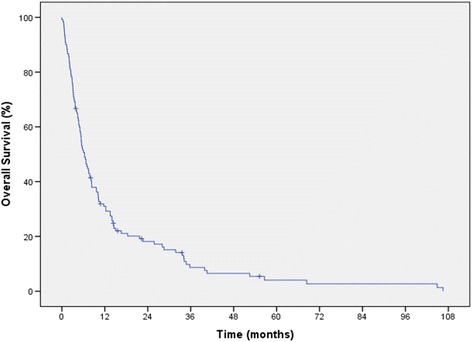
120 patients (52 females) with a median age of 72 (range 65-83) were treated. The most common histological subtypes were undifferentiated sarcoma (30%), leiomyosarcoma (27%), angiosarcoma (14%). 42% of patients had high grade tumours. 70% of patients had metastatic disease at presentation; lung metastasis being the most common disease site (72%). 80% received single agent chemotherapy, mostly with doxorubicin (60%). The median number of cycles was 2 (IQR 3). A partial response was reported in 20% of patients with disease stabilisation in a further 20%. 38% of patients were hospitalised for chemotherapy related toxicity. The median overall survival (OS) was 6.5 months (95% CI 4.7-8.3). Anaemia, lymphopenia, hypoalbuminemia, sarcoma subtype and co-morbidities were predictive for overall survival.
The overall survival for elderly patients with STS is poor but several predictive factors have been identified. Hospital admissions for chemotherapy related toxicity are common.
老年软组织肉瘤(STS)一线姑息化疗的疗效和毒性鲜有描述。
确定1998年1月至2012年1月在皇家马斯登医院接受晚期非胃肠道间质瘤STS一线化疗的65岁以上患者。回顾性收集生存及预测因素的数据。
共治疗120例患者(52例女性),中位年龄72岁(范围65 - 83岁)。最常见的组织学亚型为未分化肉瘤(30%)、平滑肌肉瘤(27%)、血管肉瘤(14%)。42%的患者肿瘤分级高。70%的患者初诊时已有转移性疾病;肺转移是最常见的转移部位(72%)。80%的患者接受单药化疗,大多使用阿霉素(60%)。中位化疗周期数为2(四分位间距3)。20%的患者有部分缓解,另有20%疾病稳定。38%的患者因化疗相关毒性住院。中位总生存期(OS)为6.5个月(95%可信区间4.7 - 8.3)。贫血、淋巴细胞减少、低白蛋白血症、肉瘤亚型及共病是总生存期的预测因素。
老年STS患者的总生存期较差,但已确定了几个预测因素。因化疗相关毒性住院很常见。