Tsai-Goodman Beverly, Zhu Meng Yuan, Al-Rujaib Mashael, Seed Mike, Macgowan Christopher K
Department of Paediatric Cardiology, Bristol Children's Hospital, University of Bristol, Bristol, United Kingdom.
Department of Paediatrics and Division of Cardiology, University of Toronto & Hospital for Sick Children, Toronto, Canada.
J Cardiovasc Magn Reson. 2015 Apr 18;17(1):30. doi: 10.1186/s12968-015-0132-2.
Phase contrast cardiovascular magnetic resonance (PC CMR) has emerged as a clinical tool for blood flow quantification but its use in the foetus has been hampered by the need for gating with the foetal heart beat. The previously described metric optimized gating (MOG) technique has been successfully used to measure foetal blood flow in late gestation foetuses on a 1.5 T CMR magnet. However, there is increasing interest in performing foetal cardiac imaging using 3.0 T CMR. We describe our pilot investigation of foetal blood flow measured using 3.0 T CMR.
Foetal blood flows were quantified in 5 subjects at late gestational age (35-38 weeks). Three were normal pregnancies and two were pregnancies with ventricular size discrepancy. Data were obtained at 1.5 T and 3.0 T using a previously described PC CMR protocol. After reconstruction using MOG, blood flow was quantified independently by two observers. Intra- and inter-observer reproducibility of flow measurements at the two field strengths was assessed by Pearson correlation coefficient (R(2)), linear regression and Bland Altman analysis.
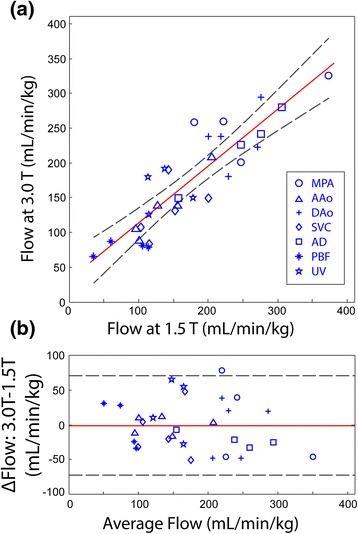
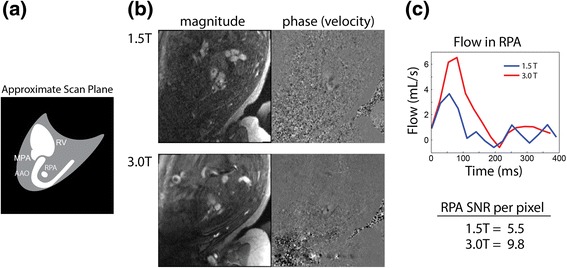
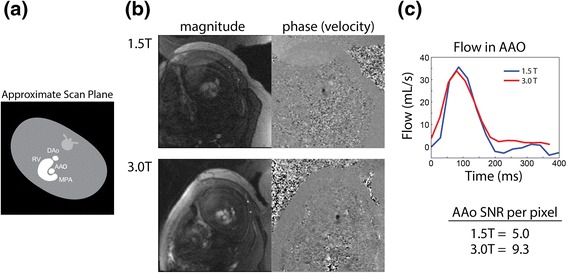
PC CMR flow measurements were obtained in 36 of 40 target vessels. Strong intra-observer agreement was obtained between measurements at each field strength (R(2) = 0.78, slope = 0.83 ± 0.11), with a mean bias of -1 ml/min/kg and 95% confidence limits of ±71 ml/min/kg. Inter-observer agreement was similarly high for measurements at both 1.5 T (R(2) = 0.86, slope = 0.95 ± 0.13, bias = 6 ± 52 ml/min/kg) and 3.0 T (R(2) = 0.88, slope = 0.94 ± 0.13, bias = 4 ± 47 ml/min/kg). Across all PC CMR measurements, SNR per pixel was expectedly higher at 3.0 T relative to 1.5 T (165 ± 50%). The relative differences in flow measurements between observers were low (range: 4-16%) except for pulmonary blood flow which showed much higher variability at 1.5 T (34%) versus that at 3.0 T (11%). This was attributed to the poorly visualized, small pulmonary vessels at 1.5 T, which made delineation inconsistent between observers.
This is the first pilot study to measure foetal blood flow using PC CMR at 3.0 T. The flow data obtained were in good correlation with those measured at 1.5 T, both within and between observers. With increased SNR at 3.0 T, smaller pulmonary vessels were better visualized which improved inter-observer agreement of associated flows.
相位对比心血管磁共振成像(PC CMR)已成为一种用于血流定量分析的临床工具,但其在胎儿检查中的应用因需要与胎儿心跳同步门控而受到限制。先前描述的度量优化门控(MOG)技术已成功用于在1.5T CMR磁体上测量晚期妊娠胎儿的血流。然而,使用3.0T CMR进行胎儿心脏成像的兴趣日益增加。我们描述了我们使用3.0T CMR测量胎儿血流的初步研究。
对5名孕晚期(35 - 38周)的受试者进行胎儿血流定量分析。其中3例为正常妊娠,2例为心室大小存在差异的妊娠。使用先前描述的PC CMR方案在1.5T和3.0T下获取数据。在使用MOG重建后,由两名观察者独立对血流进行定量分析。通过Pearson相关系数(R²)、线性回归和Bland Altman分析评估两名观察者在两种场强下血流测量的观察者内和观察者间的可重复性。
在40条目标血管中的36条获得了PC CMR血流测量值。在每个场强下的测量之间获得了观察者内的高度一致性(R² = 0.78,斜率 = 0.83±0.11),平均偏差为 -1 ml/min/kg,95%置信限为±71 ml/min/kg。在1.5T(R² = 0.86,斜率 = 0.95±0.13,偏差 = 6±52 ml/min/kg)和3.0T(R² = 0.88,斜率 = 0.94±0.13,偏差 = 4±47 ml/min/kg)下测量的观察者间一致性同样很高。在所有PC CMR测量中,相对于1.5T,3.0T时每个像素的信噪比预期更高(165±50%)。观察者之间血流测量的相对差异较低(范围:4 - 16%),但肺血流除外,其在1.5T时的变异性(34%)远高于3.0T时(11%)。这归因于1.5T时肺血管显示不佳且较小,使得观察者之间的描绘不一致。
这是第一项使用3.0T的PC CMR测量胎儿血流的初步研究。所获得的血流数据在观察者内和观察者间与在1.5T测量的数据具有良好的相关性。随着3.0T时信噪比的提高,较小的肺血管得到了更好的显示,这提高了相关血流的观察者间一致性。