Son Christina H, Law Ethel, Oh Jung Hun, Apte Aditya P, Yang T Jonathan, Riedel Elyn, Wu Abraham J, Deasy Joseph O, Goodman Karyn A
Department of Radiation Oncology, Memorial Sloan-Kettering Cancer Center, New York, New York.
Department of Medical Physics, Memorial Sloan-Kettering Cancer Center, New York, New York.
Int J Radiat Oncol Biol Phys. 2015 Jul 1;92(3):548-54. doi: 10.1016/j.ijrobp.2015.02.029. Epub 2015 Apr 28.
Although vaginal stenosis (VS) is a recognized toxicity in women who receive pelvic radiation therapy (RT), the relationship between RT dose and the volume and extent of toxicity has not been analyzed. We modeled this relationship to identify predictors of VS.
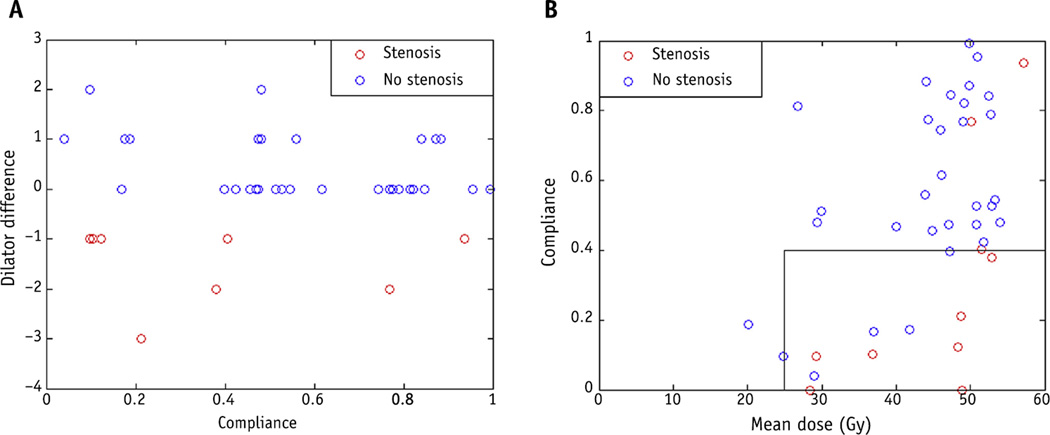
We evaluated 54 women, aged 29 to 78 years, who underwent pelvic RT for rectal or anal cancer during 2008 to 2011 and were enrolled in a prospective study evaluating vaginal dilator use. Maximum dilator size was measured before RT (baseline) and 1 month and 12 months after RT. Dilator use was initiated at 1 month. The difference (D) in dilator size before and after RT was recorded. Those with D ≤-1 were classified as having VS (n=35); those with D ≥0 were classified as having no VS (n=19 at 1 month). Dose-volume parameters were extracted, and the generalized equivalent uniform dose (gEUD) was used to build a predictive model.
The mean vaginal doses were 50.0 Gy and 36.8 Gy for anal and rectal cancer patients, respectively. One month after RT, a gEUD model using a wide range of a values suggests that sparing of vaginal volume to a low dose may be important. When gEUD (a = -1) was <35 Gy and the mean vaginal dose was <43 Gy, severe VS was reduced (P=.02). A 1-year analysis suggests increasingly negative D values with increasing mean dose. However, patients with compliance <40% were more likely to have toxicity.
Vaginal stenosis is influenced by multiple RT dose-volume characteristics. Mean dose and gEUD constraints together may reduce the risk of severe VS. Patients receiving higher mean vaginal doses should have greater compliance with dilator therapy to minimize risk of toxicity. Further validation with independent datasets is needed.
尽管阴道狭窄(VS)是接受盆腔放射治疗(RT)的女性中一种公认的毒性反应,但尚未分析放疗剂量与毒性反应的体积和范围之间的关系。我们建立了这种关系模型以识别阴道狭窄的预测因素。
我们评估了54名年龄在29至78岁之间的女性,她们在2008年至2011年期间因直肠癌或肛管癌接受了盆腔放疗,并参与了一项评估阴道扩张器使用情况的前瞻性研究。在放疗前(基线)、放疗后1个月和12个月测量最大扩张器尺寸。扩张器使用从1个月开始。记录放疗前后扩张器尺寸的差值(D)。D≤ -1的患者被归类为患有阴道狭窄(n = 35);D≥0的患者被归类为没有阴道狭窄(1个月时n = 19)。提取剂量-体积参数,并使用广义等效均匀剂量(gEUD)建立预测模型。
肛管癌和直肠癌患者的平均阴道剂量分别为50.0 Gy和36.8 Gy。放疗后1个月,使用广泛a值范围的gEUD模型表明,将阴道体积 sparing 到低剂量可能很重要。当gEUD(a = -1)<35 Gy且平均阴道剂量<43 Gy时,严重阴道狭窄减少(P = 0.02)。1年的分析表明,随着平均剂量增加,D值越来越负。然而,依从性<40%的患者更有可能出现毒性反应。
阴道狭窄受多种放疗剂量-体积特征的影响。平均剂量和gEUD限制共同作用可能降低严重阴道狭窄的风险。接受较高平均阴道剂量的患者应更好地依从扩张器治疗,以将毒性风险降至最低。需要使用独立数据集进行进一步验证。