Herrel Lindsey A, Ye Zaojun, Miller David C
Department of Urology, Dow Division of Health Services Research, University of Michigan, Ann Arbor, Michigan; Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor, Michigan.
Department of Urology, Dow Division of Health Services Research, University of Michigan, Ann Arbor, Michigan; Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor, Michigan.
J Urol. 2015 Nov;194(5):1380-5. doi: 10.1016/j.juro.2015.04.098. Epub 2015 Apr 30.
Because proposed funding cuts in the Patient Protection and Affordable Care Act may impact care for urological patients at safety net hospitals, we examined the use, outcomes and costs of inpatient urological surgery at safety net vs nonsafety net facilities prior to health care reform.
Using the Nationwide Inpatient Sample we performed a retrospective cohort study of patients who underwent inpatient urological surgeries from 2007 through 2011. We defined the safety net burden of each hospital based on the proportion of Medicaid and self-pay discharges. We examined the distribution of urological procedures performed and compared in-hospital mortality, prolonged length of stay and costs in the highest quartile of burden (safety net) vs the lowest quartile (nonsafety net).
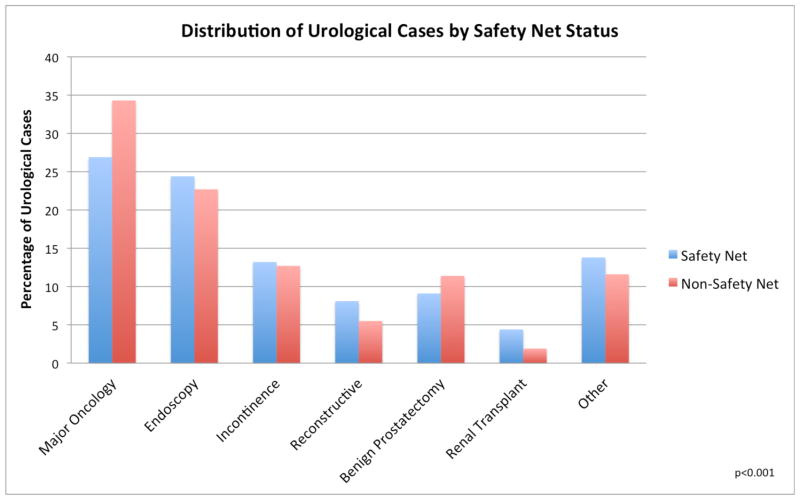
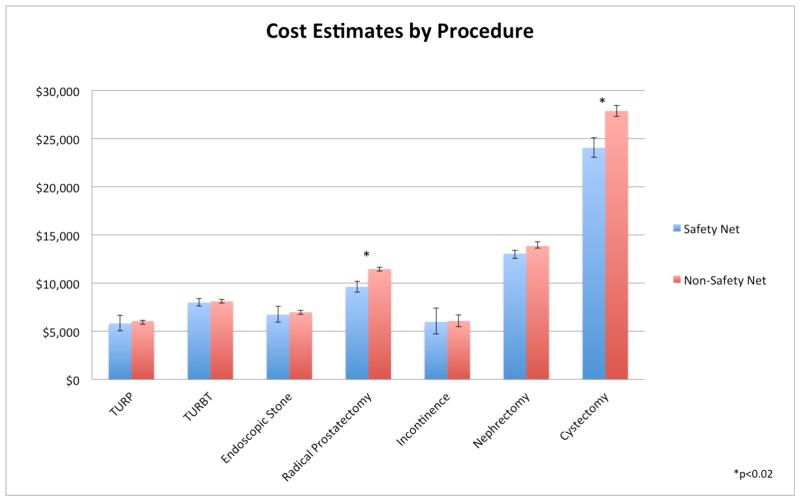
The distribution of urological procedures differed by safety net status with less benign prostate surgery (9.1% safety net vs 11.4% nonsafety net) and major cancer surgery (26.9% vs 34.3%), and more reconstructive surgery (8.1% vs 5.5%) at safety net facilities (p <0.001). Higher mortality at safety net hospitals was seen for nephrectomy (OR 1.68, 95% CI 1.15-2.45) and transurethral resection of the prostate (OR 2.17, 95% CI 1.22-3.87). Patients in safety net hospitals demonstrated greater prolonged length of stay after endoscopic stone surgery (OR 1.20, 95% CI 1.01-1.41). Costs were similar across procedures except for radical prostatectomy and cystectomy. For these procedures the average admission was more expensive at nonsafety net facilities (prostatectomy $11,457 vs $9,610 and cystectomy $27,875 vs $24,048, each p <0.02).
Reductions in funding to safety net hospitals with health care reform could adversely impact access to care for patients with a broad range of urological conditions, potentially exacerbating existing disparities for vulnerable populations served by these facilities.
鉴于《患者保护与平价医疗法案》中提议的资金削减可能会影响安全网医院对泌尿外科患者的治疗,我们在医疗改革之前,对安全网医院与非安全网医院的住院泌尿外科手术的使用情况、治疗结果及费用进行了研究。
利用全国住院样本,我们对2007年至2011年期间接受住院泌尿外科手术的患者进行了一项回顾性队列研究。我们根据医疗补助和自费出院患者的比例来确定每家医院的安全网负担情况。我们研究了所实施的泌尿外科手术的分布情况,并比较了负担最高四分位数(安全网)与最低四分位数(非安全网)患者的院内死亡率、住院时间延长情况及费用。
泌尿外科手术的分布因安全网状况而异,在安全网医院,良性前列腺手术(9.1%的安全网医院 vs 11.4%的非安全网医院)和重大癌症手术(26.9% vs 34.3%)较少,而重建手术较多(8.1% vs 5.5%)(p<0.001)。在安全网医院,肾切除术(比值比1.68,95%可信区间1.15 - 2.45)和经尿道前列腺切除术(比值比2.17,95%可信区间1.22 - 3.87)的死亡率较高。安全网医院的患者在内镜下结石手术后住院时间延长的情况更明显(比值比1.20,95%可信区间1.01 - 1.41)。除根治性前列腺切除术和膀胱切除术外,各手术的费用相似。对于这些手术,非安全网医院的平均住院费用更高(前列腺切除术分别为11,457美元 vs 9,610美元,膀胱切除术分别为27,875美元 vs 24,048美元,p均<0.02)。
医疗改革中对安全网医院资金的削减可能会对患有多种泌尿外科疾病的患者获得治疗产生不利影响,可能会加剧这些机构所服务的弱势群体中现有的差距。