Kertai Miklos D, Li Yi-Ju, Li Yen-Wei, Ji Yunqi, Alexander John, Newman Mark F, Smith Peter K, Joseph Diane, Mathew Joseph P, Podgoreanu Mihai V
Division of Cardiothoracic Anesthesiology, Duke University, Durham, North Carolina, USA.
Department of Biostatistics and Bioinformatics, Duke University, Durham, North Carolina, USA Duke Molecular Physiology Institute; Duke University, Durham, North Carolina, USA.
BMJ Open. 2015 May 6;5(5):e006920. doi: 10.1136/bmjopen-2014-006920.
Identification of patient subpopulations susceptible to develop myocardial infarction (MI) or, conversely, those displaying either intrinsic cardioprotective phenotypes or highly responsive to protective interventions remain high-priority knowledge gaps. We sought to identify novel common genetic variants associated with perioperative MI in patients undergoing coronary artery bypass grafting using genome-wide association methodology.
107 secondary and tertiary cardiac surgery centres across the USA.
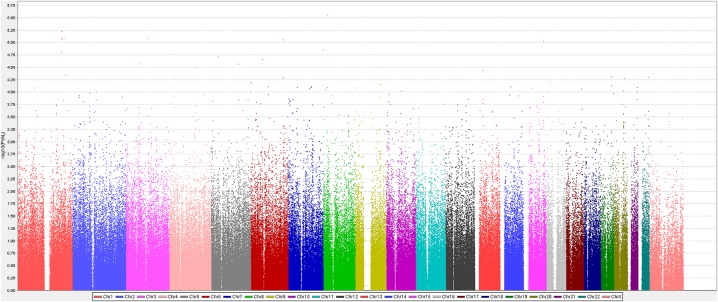
We conducted a stage I genome-wide association study (GWAS) in 1433 ethnically diverse patients of both genders (112 cases/1321 controls) from the Genetics of Myocardial Adverse Outcomes and Graft Failure (GeneMAGIC) study, and a stage II analysis in an expanded population of 2055 patients (225 cases/1830 controls) combined from the GeneMAGIC and Duke Perioperative Genetics and Safety Outcomes (PEGASUS) studies. Patients undergoing primary non-emergent coronary bypass grafting were included.
The primary outcome variable was perioperative MI, defined as creatine kinase MB isoenzyme (CK-MB) values ≥10× upper limit of normal during the first postoperative day, and not attributable to preoperative MI. Secondary outcomes included postoperative CK-MB as a quantitative trait, or a dichotomised phenotype based on extreme quartiles of the CK-MB distribution.
Following quality control and adjustment for clinical covariates, we identified 521 single nucleotide polymorphisms in the stage I GWAS analysis. Among these, 8 common variants in 3 genes or intergenic regions met p<10(-5) in stage II. A secondary analysis using CK-MB as a quantitative trait (minimum p=1.26×10(-3) for rs609418), or a dichotomised phenotype based on extreme CK-MB values (minimum p=7.72×10(-6) for rs4834703) supported these findings. Pathway analysis revealed that genes harbouring top-scoring variants cluster in pathways of biological relevance to extracellular matrix remodelling, endoplasmic reticulum-to-Golgi transport and inflammation.
Using a two-stage GWAS and pathway analysis, we identified and prioritised several potential susceptibility loci for perioperative MI.
确定易发生心肌梗死(MI)的患者亚群,或者相反,确定那些具有内在心脏保护表型或对保护干预措施反应高度敏感的亚群,仍然是亟待填补的重要知识空白。我们试图采用全基因组关联方法,确定冠状动脉搭桥手术患者围手术期MI相关的新型常见基因变异。
美国107家二级和三级心脏外科中心。
我们在心肌不良结局与移植物衰竭遗传学(GeneMAGIC)研究中的1433名不同种族的男女患者(112例病例/1321例对照)中进行了第一阶段全基因组关联研究(GWAS),并在由GeneMAGIC和杜克围手术期遗传学与安全结局(PEGASUS)研究合并的2055名患者(225例病例/1830例对照)的扩大队列中进行了第二阶段分析。纳入接受择期非急诊冠状动脉搭桥手术的患者。
主要结局变量为围手术期MI,定义为术后第1天肌酸激酶MB同工酶(CK-MB)值≥正常上限的10倍,且与术前MI无关。次要结局包括术后CK-MB作为定量性状,或基于CK-MB分布的极端四分位数的二分法表型。
经过质量控制和临床协变量调整后,我们在第一阶段GWAS分析中鉴定出521个单核苷酸多态性。其中,3个基因或基因间区域的8个常见变异在第二阶段满足p< /sup>10-5。使用CK-MB作为定量性状的二次分析(rs609418的最小p=1.26×10-3),或基于极端CK-MB值的二分法表型(rs4834703的最小p=7.72×10-6)支持了这些发现。通路分析显示,携带得分最高变异的基因聚集在与细胞外基质重塑、内质网到高尔基体转运和炎症生物学相关的通路中。
通过两阶段GWAS和通路分析,我们确定了几个围手术期MI的潜在易感位点并对其进行了排序。