1 Helen Wills Neuroscience Institute, University of California, Berkeley, Berkeley CA, USA
1 Helen Wills Neuroscience Institute, University of California, Berkeley, Berkeley CA, USA 2 Lawrence Berkeley National Laboratory, Berkeley, California, USA 3 Memory and Aging Centre, Department of Neurology, University of California, San Francisco, USA.
Brain. 2015 Jul;138(Pt 7):2020-33. doi: 10.1093/brain/awv112. Epub 2015 May 6.
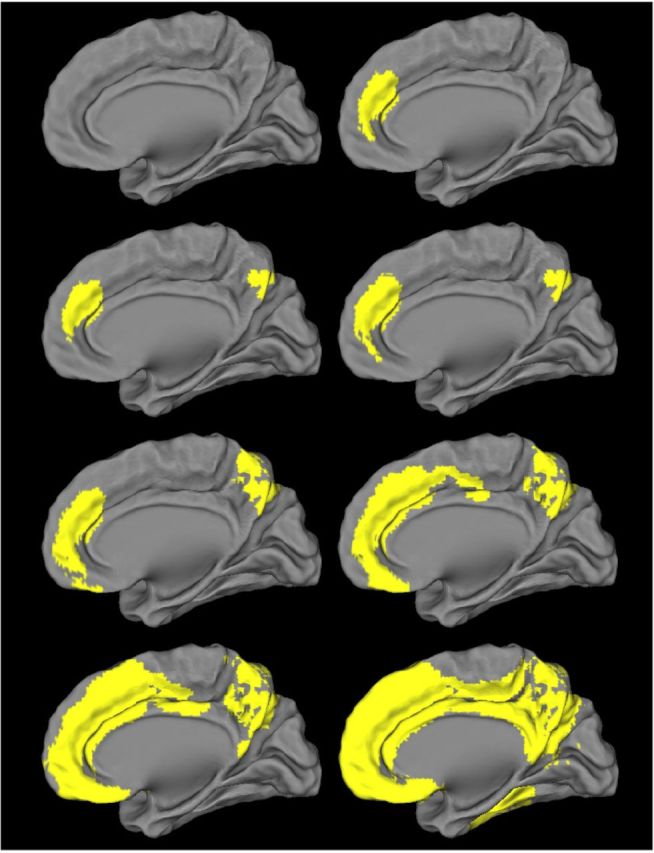
Amyloid-β, a hallmark of Alzheimer's disease, begins accumulating up to two decades before the onset of dementia, and can be detected in vivo applying amyloid-β positron emission tomography tracers such as carbon-11-labelled Pittsburgh compound-B. A variety of thresholds have been applied in the literature to define Pittsburgh compound-B positron emission tomography positivity, but the ability of these thresholds to detect early amyloid-β deposition is unknown, and validation studies comparing Pittsburgh compound-B thresholds to post-mortem amyloid burden are lacking. In this study we first derived thresholds for amyloid positron emission tomography positivity using Pittsburgh compound-B positron emission tomography in 154 cognitively normal older adults with four complementary approaches: (i) reference values from a young control group aged between 20 and 30 years; (ii) a Gaussian mixture model that assigned each subject a probability of being amyloid-β-positive or amyloid-β-negative based on Pittsburgh compound-B index uptake; (iii) a k-means cluster approach that clustered subjects into amyloid-β-positive or amyloid-β-negative based on Pittsburgh compound-B uptake in different brain regions (features); and (iv) an iterative voxel-based analysis that further explored the spatial pattern of early amyloid-β positron emission tomography signal. Next, we tested the sensitivity and specificity of the derived thresholds in 50 individuals who underwent Pittsburgh compound-B positron emission tomography during life and brain autopsy (mean time positron emission tomography to autopsy 3.1 ± 1.8 years). Amyloid at autopsy was classified using Consortium to Establish a Registry for Alzheimer's Disease (CERAD) criteria, unadjusted for age. The analytic approaches yielded low thresholds (standard uptake value ratiolow = 1.21, distribution volume ratiolow = 1.08) that represent the earliest detectable Pittsburgh compound-B signal, as well as high thresholds (standard uptake value ratiohigh = 1.40, distribution volume ratiohigh = 1.20) that are more conservative in defining Pittsburgh compound-B positron emission tomography positivity. In voxel-wise contrasts, elevated Pittsburgh compound-B retention was first noted in the medial frontal cortex, then the precuneus, lateral frontal and parietal lobes, and finally the lateral temporal lobe. When compared to post-mortem amyloid burden, low proposed thresholds were more sensitive than high thresholds (sensitivities: distribution volume ratiolow 81.0%, standard uptake value ratiolow 83.3%; distribution volume ratiohigh 61.9%, standard uptake value ratiohigh 62.5%) for CERAD moderate-to-frequent neuritic plaques, with similar specificity (distribution volume ratiolow 95.8%; standard uptake value ratiolow, distribution volume ratiohigh and standard uptake value ratiohigh 100.0%). A receiver operator characteristic analysis identified optimal distribution volume ratio (1.06) and standard uptake value ratio (1.20) thresholds that were nearly identical to the a priori distribution volume ratiolow and standard uptake value ratiolow. In summary, we found that frequently applied thresholds for Pittsburgh compound-B positivity (typically at or above distribution volume ratiohigh and standard uptake value ratiohigh) are overly stringent in defining amyloid positivity. Lower thresholds in this study resulted in higher sensitivity while not compromising specificity.
淀粉样蛋白-β(amyloid-β)是阿尔茨海默病的一个标志,早在痴呆症发病前 20 年就开始积累,并且可以通过碳-11 标记的匹兹堡化合物-B 等淀粉样蛋白-β正电子发射断层扫描示踪剂在体内检测到。文献中已经应用了多种阈值来定义匹兹堡化合物-B 正电子发射断层扫描阳性,但这些阈值检测早期淀粉样蛋白-β沉积的能力尚不清楚,并且缺乏将匹兹堡化合物-B 阈值与死后淀粉样蛋白负担进行比较的验证研究。在这项研究中,我们首先使用匹兹堡化合物-B 正电子发射断层扫描,通过四种互补方法为 154 名认知正常的老年人确定了淀粉样蛋白正电子发射断层扫描阳性的阈值:(i)来自 20 至 30 岁年轻对照组的参考值;(ii)基于匹兹堡化合物-B 指数摄取,为每个受试者分配一个为淀粉样蛋白-β阳性或淀粉样蛋白-β阴性的概率的高斯混合模型;(iii)基于不同大脑区域(特征)中匹兹堡化合物-B 摄取的聚类方法,将受试者聚类为淀粉样蛋白-β阳性或淀粉样蛋白-β阴性;(iv)进一步探索早期淀粉样蛋白正电子发射断层扫描信号空间模式的迭代体素分析。接下来,我们在 50 名接受匹兹堡化合物-B 正电子发射断层扫描的个体(正电子发射断层扫描与尸检之间的平均时间为 3.1±1.8 年)中测试了得出的阈值的敏感性和特异性。使用 Consorcium to Establish a Registry for Alzheimer's Disease(CERAD)标准对死后淀粉样蛋白进行分类,未对年龄进行调整。分析方法得出的低阈值(标准摄取比值低=1.21,分布容积比值低=1.08)代表最早可检测到的匹兹堡化合物-B 信号,以及更高的阈值(标准摄取比值高=1.40,分布容积比值高=1.20),在定义匹兹堡化合物-B 正电子发射断层扫描阳性时更为保守。在体素对比中,内侧额皮质首先出现匹兹堡化合物-B 保留增加,然后是楔前叶、外侧额叶和顶叶,最后是外侧颞叶。与死后淀粉样蛋白负担相比,低提议的阈值对 CERAD 中度至频繁的神经突斑块的敏感性高于高阈值(分布容积比值低为 81.0%,标准摄取比值低为 83.3%;分布容积比值高为 61.9%,标准摄取比值高为 62.5%),特异性相似(分布容积比值低为 95.8%,标准摄取比值低为 100.0%)。接收器操作特征分析确定了最佳的分布容积比(1.06)和标准摄取比值(1.20)阈值,与先验的分布容积比低和标准摄取比值低几乎相同。总之,我们发现,匹兹堡化合物-B 阳性的常用阈值(通常为分布容积比高和标准摄取比值高)在定义淀粉样蛋白阳性时过于严格。本研究中的较低阈值导致了更高的敏感性,同时不影响特异性。