Kuriyama Satoru, Maruyama Yukio, Nishio Shinichiro, Takahashi Yasuhito, Kidoguchi Satoshi, Kobayashi Chisa, Takahashi Daisuke, Sugano Naoki, Hosoya Tatsuo, Yokoo Takashi
Division of Nephrology and Hypertension, Department of Internal Medicine, Jikei University School of Medicine, 3-25-8, Nishi-shinbashi, Minato-ku, Tokyo, 105-8461, Japan.
Department of Pathophysiology and Therapy in Chronic Kidney Disease, Jikei University School of Medicine, Tokyo, Japan.
Clin Exp Nephrol. 2015 Dec;19(6):1127-34. doi: 10.1007/s10157-015-1120-4. Epub 2015 May 13.
Uric acid (UA) levels correlate positively with the prevalence of chronic kidney disease (CKD) and/or hypertension. We tested the hypothesis that UA may also have a link to a new incidence of CKD and hypertension.
Study design is a cohort study and the predictor is UA levels. Of the 15,470 screened cases, 8223 participants without CKD were eligible for the analysis of the incidence of CKD. Among these CKD candidates, 7569 participants were eligible for the analysis of the new development of hypertension. The observation period was 4 years.
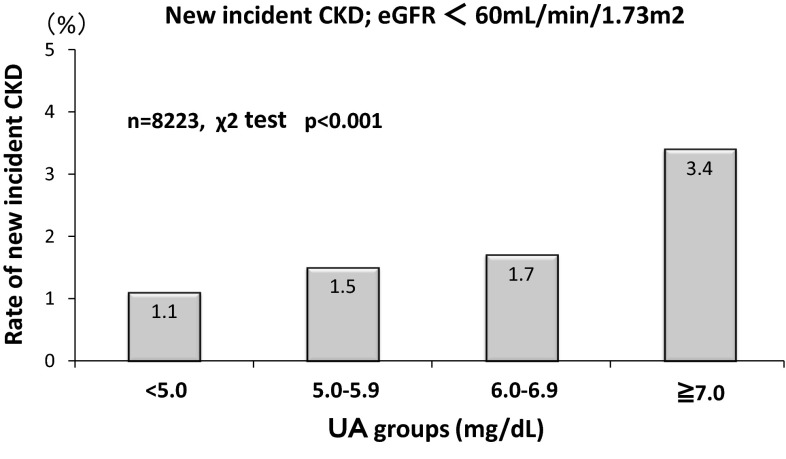
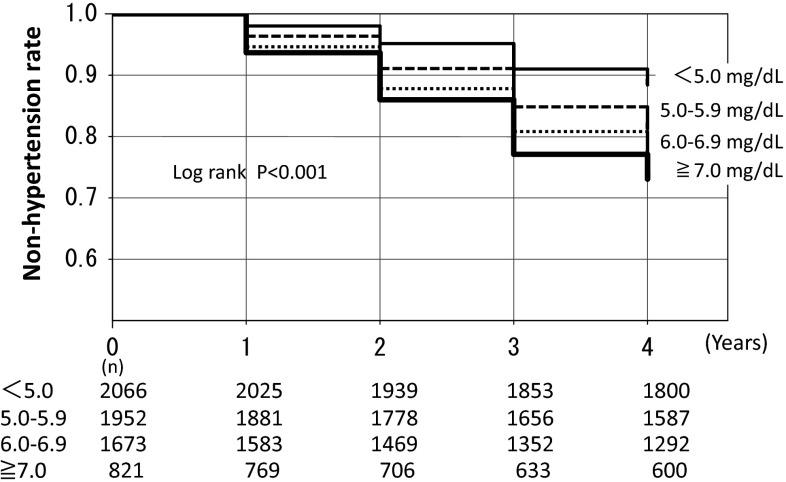
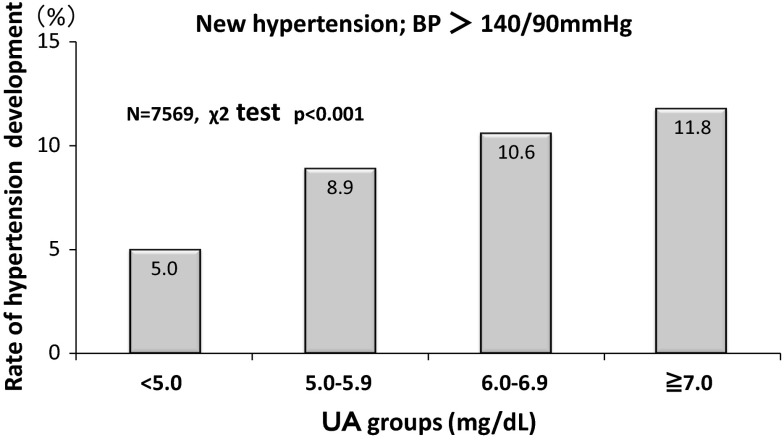
Relationship of UA with new cases of CKD. Higher UA levels had a closer association with the new development of CKD; 1.1 % (UA < 5 mg/dL), 1.5 % (5.0-5.9 mg/dL), 1.7 % (6.0-6.9 mg/dL), and 3.4 % (≧7 mg/dL), respectively (p < 0.001 by the Chi-square test). Cox proportional hazard analysis showed that the estimates of the CKD development were eGFR [Hazard Ratio (HR) 0.816, 95 % confidence intervals (CI) 0.791-0.840] and male gender (HR 0.562, 95 % CI 0.322-0.982). UA levels and new development of hypertension. Higher UA levels had a closer association with the new development of hypertension; 5.0 % (UA < 5 mg/dL), 8.9 % (5.0-5.9 mg/dL), 10.6 % (6.0-6.9 mg/dL), and 11.8 % (≧7 mg/dL), respectively (p < 0.001 by the Chi-square test). Cox proportional hazard analysis showed that the estimates of the hypertension development were BMI (HR 1.190, 95 % CI 1.155-1.226), age (HR 1.021, 95 % CI 1.010-1.032), HDL-cholesterol (HR 1.013, 95 % CI 1.007-1.019), male gender (HR 1.791, 95 % CI 1.338-2.395), UA level (HR 1.112, 95 % CI 1.024-1.207), and eGFR (HR 1008, 95 % CI 1.002-1.013). Furthermore, the logistic analysis showed that the odds ratio (OR) to estimate hypertension in the high UA group (UA ≧ 7 mg/dL; OR 1.33, 95 % CI 1.01-1.80) was greater than that in the low UA group (UA < 5 mg/dL). Kaplan-Meier analysis also confirmed the finding that the higher the UA levels the greater the hypertension development (p < 0.001 by the Log-rank test and Cox proportional hazard analysis).
High UA levels are associated with the new development of hypertension, but not with the incidence of CKD.
尿酸(UA)水平与慢性肾脏病(CKD)和/或高血压的患病率呈正相关。我们检验了尿酸可能也与CKD和高血压的新发有关这一假设。
研究设计为队列研究,预测指标为尿酸水平。在15470例筛查病例中,8223例无CKD的参与者符合CKD发病率分析的条件。在这些CKD候选者中,7569例参与者符合高血压新发情况分析的条件。观察期为4年。
尿酸与CKD新发病例的关系。较高的尿酸水平与CKD的新发密切相关;分别为1.1%(尿酸<5mg/dL)、1.5%(5.0 - 5.9mg/dL)、1.7%(6.0 - 6.9mg/dL)和3.4%(≥7mg/dL)(卡方检验p<0.001)。Cox比例风险分析显示,CKD发生的估计因素为估算肾小球滤过率(eGFR)[风险比(HR)0.816,95%置信区间(CI)0.791 - 0.840]和男性性别(HR 0.562,95%CI 0.322 - 0.982)。尿酸水平与高血压的新发。较高的尿酸水平与高血压的新发密切相关;分别为5.0%(尿酸<5mg/dL)、8.9%(5.0 - 5.9mg/dL)、10.6%(6.0 - 6.9mg/dL)和11.8%(≥7mg/dL)(卡方检验p<0.001)。Cox比例风险分析显示,高血压发生的估计因素为体重指数(BMI)(HR