Choi Hyuk Joong, Kim Young-Min, Oh Young Min, Kang Hyung Goo, Yim Hyun Woo, Jeong Seung Hee
Department of Emergency Medicine, College of Medicine, Hanyang University, Seoul, Korea.
Department of Emergency Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
BMJ Open. 2015 May 11;5(5):e007884. doi: 10.1136/bmjopen-2015-007884.
To evaluate whether the use of a GlideScope video laryngoscope (GVL) improves first-attempt intubation success compared with the Macintosh laryngoscope (MAC) in the emergency department (ED).
A propensity score-matched analysis of data from a prospective multicentre ED airway registry-the Korean Emergency Airway Management Registry (KEAMR).
4 academic EDs located in a metropolitan city and a province in South Korea.
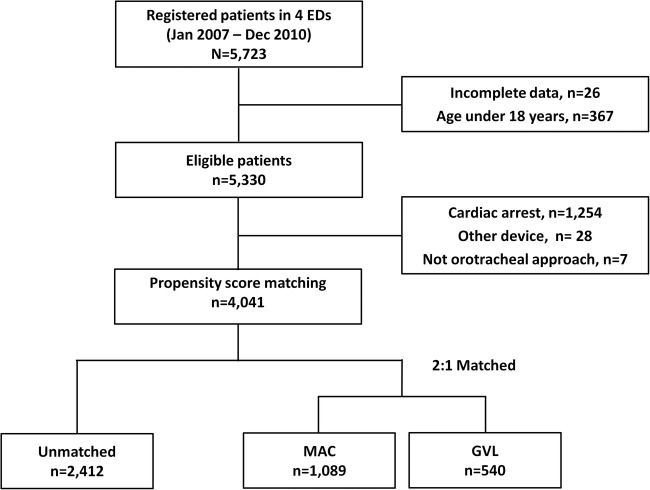
A total of 4041 adult patients without cardiac arrest who underwent emergency intubation from January 2007 to December 2010.
The primary and secondary outcomes were successful first intubation attempt and intubation failure, respectively. To reduce the selection bias and potential confounding effects, we rigorously adjusted for the baseline differences between two groups using a propensity score matching.
Of the 4041 eligible patients, a GVL was initially used in 540 patients (13.4%). Using 1:2 propensity score matching, 363 and 726 patients were assigned to the GVL and MAC groups, respectively. The adjusted relative risks (95% CIs) for the first-attempt success rates with a GVL compared with a MAC were 0.76 (0.56 to 1.04; p=0.084) and the respective intubation failure rates 1.03(0.99 to 1.07; p=0.157). Regarding the subgroups, the first-attempt success of the senior residents and attending physicians was lower with the GVL (0.47 (0.23 to 0.98), p=0.043). In the patients with slight intubation difficulty, the first-attempt success was lower (0.60 (0.41 to 0.88), p=0.008) and the intubation failure was higher with the GVL (1.07 (1.02 to 1.13), p=0.008).
In this propensity score-matched analysis of data from a prospective multicentre ED airway registry, the overall first-attempt intubation success and failure rates did not differ significantly between GVL and MAC in the ED setting. Further randomised controlled trials are needed to confirm our findings.
评估在急诊科(ED)使用GlideScope视频喉镜(GVL)与Macintosh喉镜(MAC)相比是否能提高首次气管插管成功率。
对来自前瞻性多中心ED气道登记处——韩国急诊气道管理登记处(KEAMR)的数据进行倾向评分匹配分析。
位于韩国一个大城市和一个省份的4家学术性急诊科。
2007年1月至2010年12月期间共4041例未发生心脏骤停且接受急诊气管插管的成年患者。
主要和次要观察指标分别为首次气管插管成功和气管插管失败。为减少选择偏倚和潜在的混杂效应,我们使用倾向评分匹配对两组之间的基线差异进行了严格校正。
在4041例符合条件的患者中,最初有540例(13.4%)使用了GVL。采用1:2倾向评分匹配,分别将363例和726例患者分配至GVL组和MAC组。与MAC相比,GVL首次尝试成功率的校正相对风险(95%CI)为0.76(0.56至1.04;p = 0.084),相应的气管插管失败率为1.03(0.99至1.07;p = 0.157)。在亚组分析中,住院医师和主治医师使用GVL时首次尝试成功率较低(0.47(0.23至0.98),p = 0.043)。在插管难度较小的患者中,GVL的首次尝试成功率较低(0.60(0.41至0.88),p = 0.008),气管插管失败率较高(1.07(1.02至1.13),p = 0.008)。
在这项对前瞻性多中心ED气道登记处数据进行的倾向评分匹配分析中,在ED环境中,GVL和MAC的总体首次气管插管成功率和失败率无显著差异。需要进一步的随机对照试验来证实我们的研究结果。