Broyles Lauren M, Wieland Melissa E, Confer Andrea L, DiNardo Monica M, Kraemer Kevin L, Hanusa Barbara H, Youk Ada O, Gordon Adam J, Sevick Mary Ann
Center for Health Equity Research and Promotion, Veterans Affairs (VA) Pittsburgh Healthcare System, University Drive C (151C), Pittsburgh, PA, 15240, USA.
Division of General Internal Medicine, Department of Medicine, School of Medicine, University of Pittsburgh, 230 McKee Place, Suite 600, Pittsburgh, PA, 15213, USA.
Addict Sci Clin Pract. 2015 May 13;10(1):13. doi: 10.1186/s13722-015-0033-6.
Various hospital accreditation and quality assurance entities in the United States have approved and endorsed performance measures promoting alcohol brief intervention (BI) for hospitalized individuals who screen positive for unhealthy alcohol use, the spectrum of use ranging from hazardous use to alcohol use disorders. These performance measures have been controversial due to the limited and equivocal evidence for the efficacy of BI among hospitalized individuals. The few BI trials conducted with hospital inpatients vary widely in methodological quality. While the majority of these studies indicate limited to no effects of BI in this population, none have been designed to account for the most pervasive methodological issue in BI studies presumed to drive study findings towards the null: assessment reactivity (AR).
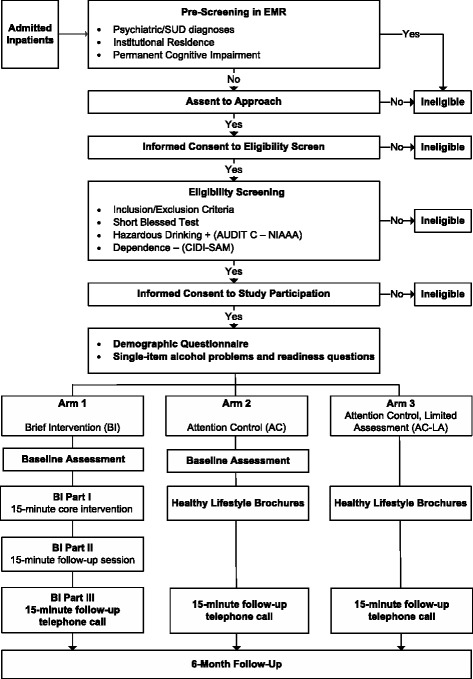
METHODS/DESIGN: This is a three-arm, single-site, randomized controlled trial of BI for hospitalized patients at a large academic medical center affiliated with the U.S. Department of Veterans Affairs who use alcohol at hazardous levels but do not have an alcohol use disorder. Participants are randomized to one of three study conditions. Study Arm 1 receives a three-part alcohol BI. Study Arm 2 receives attention control. To account for potential AR, Study Arm 3 receives AC with limited assessment. Primary outcomes will include the number of standard drinks/week and binge drinking episodes reported in the 30-day period prior to a final measurement visit obtained 6 months after hospital discharge. Additional outcomes will include readiness to change drinking behavior and number of adverse consequences of alcohol use. To assess differences in primary outcomes across the three arms, we will use mixed-effects regression models that account for a patient's repeated measures over the timepoints and clustering within medical units. Intervention implementation will be assessed by: a) review of intervention audio recordings to characterize barriers to intervention fidelity; and b) feasibility of participant recruitment, enrollment, and follow-up.
The results of this methodologically rigorous trial will provide greater justification for or against the use of BI performance measures in the inpatient setting and inform organizational responses to BI-related hospital accreditation and performance measures.
NCT01602172.
美国的各种医院认证和质量保证机构已批准并认可了一些绩效指标,这些指标旨在推动对酒精使用不健康(使用范围从危险使用到酒精使用障碍)筛查呈阳性的住院患者进行酒精简短干预(BI)。由于关于住院患者中BI疗效的证据有限且不明确,这些绩效指标一直存在争议。针对住院患者进行的少数BI试验在方法学质量上差异很大。虽然这些研究中的大多数表明BI对该人群的影响有限或没有影响,但没有一项研究旨在解决BI研究中最普遍的方法学问题,即评估反应性(AR),而这一问题被认为会使研究结果趋于无效。
方法/设计:这是一项在一家隶属于美国退伍军人事务部的大型学术医疗中心进行的三臂、单中心随机对照试验,针对的是酒精使用处于危险水平但无酒精使用障碍的住院患者。参与者被随机分配到三种研究条件之一。研究组1接受三部分酒精BI。研究组2接受注意力控制。为了考虑潜在的AR,研究组3接受有限评估的注意力控制。主要结局将包括出院6个月后在最后一次测量访视前30天内报告的每周标准饮酒量和暴饮次数。其他结局将包括改变饮酒行为的意愿以及酒精使用的不良后果数量。为了评估三个研究组在主要结局上的差异,我们将使用混合效应回归模型,该模型考虑了患者在各个时间点的重复测量以及医疗单位内的聚类情况。干预实施情况将通过以下方式进行评估:a)审查干预录音以确定干预保真度的障碍;b)参与者招募、入组和随访的可行性。
这项方法学严谨的试验结果将为在住院环境中使用或不使用BI绩效指标提供更有力的依据,并为组织对与BI相关的医院认证和绩效指标的应对措施提供参考。
NCT01602172。