Desai Rishi J, Huybrechts Krista F, Hernandez-Diaz Sonia, Mogun Helen, Patorno Elisabetta, Kaltenbach Karol, Kerzner Leslie S, Bateman Brian T
Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, MA 02120, USA
Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, MA 02120, USA.
BMJ. 2015 May 14;350:h2102. doi: 10.1136/bmj.h2102.
To provide absolute and relative risk estimates of neonatal abstinence syndrome (NAS) based on duration and timing of prescription opioid use during pregnancy in the presence or absence of additional NAS risk factors of history of opioid misuse or dependence, misuse of other substances, non-opioid psychotropic drug use, and smoking.
Observational cohort study.
Medicaid data from 46 US states.
Pregnant women filling at least one prescription for an opioid analgesic at any time during pregnancy for whom opioid exposure characteristics including duration of therapy: short term (<30 days) or long term (≥ 30 days); timing of use: early use (only in the first two trimesters) or late use (extending into the third trimester); and cumulative dose (in morphine equivalent milligrams) were assessed.
Diagnosis of NAS in liveborn infants.
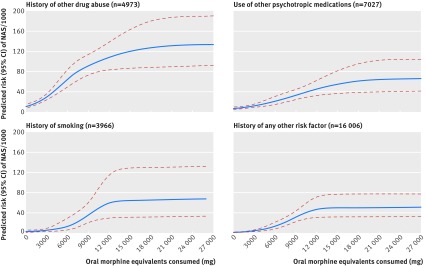
1705 cases of NAS were identified among 290,605 pregnant women filling opioid prescriptions, corresponding to an absolute risk of 5.9 per 1000 deliveries (95% confidence interval 5.6 to 6.2). Long term opioid use during pregnancy resulted in higher absolute risk of NAS per 1000 deliveries in the presence of additional risk factors of known opioid misuse (220.2 (200.8 to 241.0)), alcohol or other drug misuse (30.8 (26.1 to 36.0)), exposure to other psychotropic medications (13.1 (10.6 to 16.1)), and smoking (6.6 (4.3 to 9.6)) than in the absence of any of these risk factors (4.2 (3.3 to 5.4)). The corresponding risk estimates for short term use were 192.0 (175.8 to 209.3), 7.0 (6.0 to 8.2), 2.0 (1.5 to 2.6), 1.5 (1.0 to 2.0), and 0.7 (0.6 to 0.8) per 1000 deliveries, respectively. In propensity score matched analyses, long term prescription opioid use compared with short term use and late use compared with early use in pregnancy demonstrated greater risk of NAS (risk ratios 2.05 (95% confidence interval 1.81 to 2.33) and 1.24 (1.12 to 1.38), respectively).
Use of prescription opioids during pregnancy is associated with a low absolute risk of NAS in the absence of additional risk factors. Long term use compared with short term use and late use compared with early use of prescription opioids are associated with increased NAS risk independent of additional risk factors.
根据孕期处方阿片类药物使用的持续时间和时间,在存在或不存在阿片类药物滥用或依赖史、其他物质滥用、非阿片类精神药物使用和吸烟等额外新生儿戒断综合征(NAS)风险因素的情况下,提供NAS的绝对和相对风险估计。
观察性队列研究。
来自美国46个州的医疗补助数据。
孕期任何时间至少开具过一张阿片类镇痛药处方的孕妇,评估其阿片类药物暴露特征,包括治疗持续时间:短期(<30天)或长期(≥30天);使用时间:早期使用(仅在前两个孕期)或晚期使用(持续到第三个孕期);以及累积剂量(以吗啡当量毫克计)。
活产婴儿的NAS诊断。
在290,605名开具阿片类药物处方的孕妇中,共识别出1705例NAS病例,相当于每1000例分娩的绝对风险为5.9(95%置信区间5.6至6.2)。孕期长期使用阿片类药物,在存在已知阿片类药物滥用(220.2(200.8至241.0))、酒精或其他药物滥用(30.8(26.1至36.0))、接触其他精神药物(13.1(10.6至16.1))和吸烟(6.6(4.3至9.6))等额外风险因素时,每1000例分娩的NAS绝对风险高于不存在任何这些风险因素时(4.2(3.3至5.4))。短期使用的相应风险估计分别为每1000例分娩192.0(从统计学角度来说,175.8至209.3)、7.0(6.0至8.2)、2.0(1.5至2.6)、1.5(1.0至2.0)和0.7(0.6至0.8)。在倾向评分匹配分析中,孕期长期使用处方阿片类药物与短期使用相比,以及晚期使用与早期使用相比,显示出更高的NAS风险(风险比分别为2.05(95%置信区间1.81至2.33)和1.24(1.12至1.38))。
在不存在额外风险因素的情况下,孕期使用处方阿片类药物与NAS的绝对风险较低相关。与短期使用相比,长期使用处方阿片类药物,以及与早期使用相比,晚期使用处方阿片类药物,与NAS风险增加相关,且与额外风险因素无关。