Habayeb H, Sajin B, Patel K, Grundy C, Al-Dujaili A, Van de Velde S
Ashford & St. Peter's Hospitals NHS Foundation Trust, Guildford Road, Chertsey, KT16 0PZ, Surrey, UK,
Eur J Clin Microbiol Infect Dis. 2015 Aug;34(8):1693-9. doi: 10.1007/s10096-015-2406-x. Epub 2015 May 19.
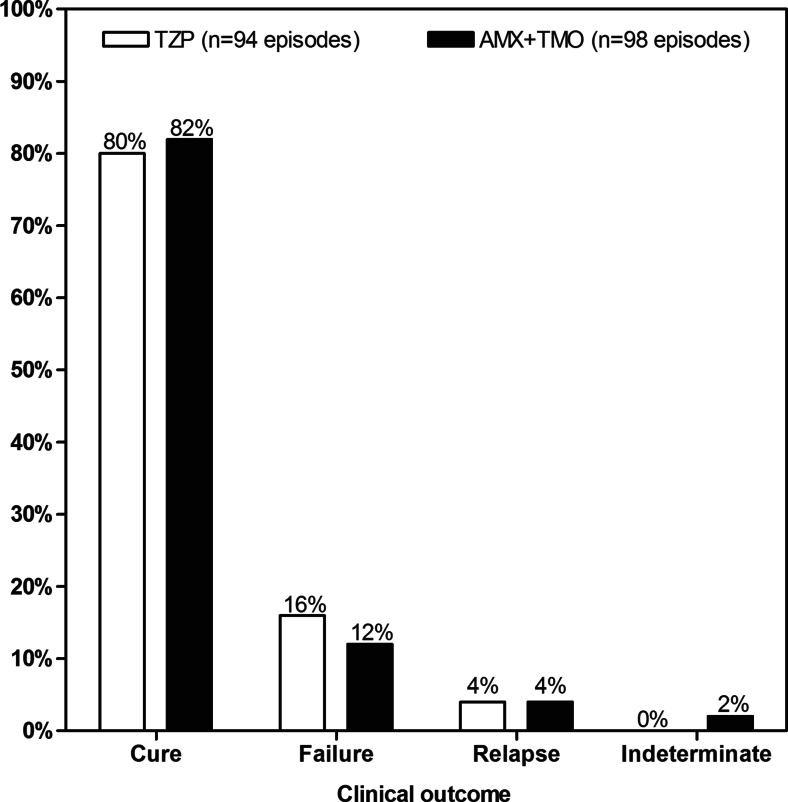
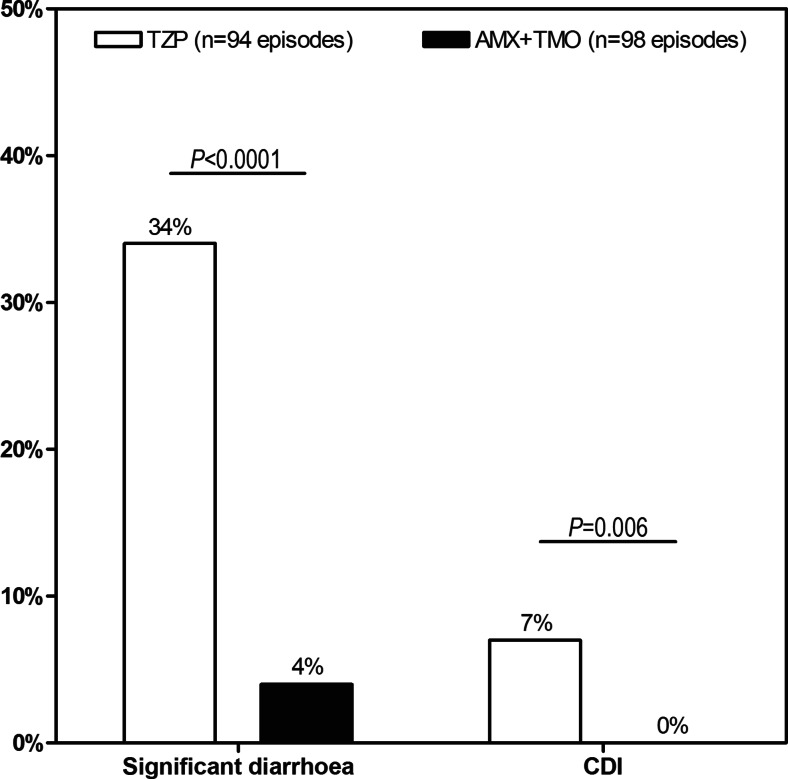
A formulary decision was made at a large provider of acute hospital services in Surrey to replace piperacillin/tazobactam with amoxicillin+temocillin for the empiric treatment of severe hospital-acquired pneumonia. This decision was made because the use of broad-spectrum-β-lactam antibiotics is a known risk factor for Clostridium difficile infection (CDI) and for the selection of resistance. After the antibiotic formulary was changed, a retrospective audit was conducted to assess the effect of this change. Data from patients hospitalised between January 2011 and July 2012 for severe hospital-acquired pneumonia and treated empirically with piperacillin/tazobactam or amoxicillin+temocillin were reviewed retrospectively. Clinical characteristics of patients, data related to the episode of pneumonia, clinical success and incidence of significant diarrhoea and CDI were analysed. One hundred ninety-two episodes of severe hospital-acquired pneumonia in 188 patients were identified from hospital records. Ninety-eight patients received piperacillin/tazobactam and 94 amoxicillin+temocillin. At baseline, the two treatment groups were comparable, except that more patients with renal insufficiency were treated with piperacillin/tazobactam. Clinical success was comparable (80 versus 82 %; P = 0.86), but differences were observed between piperacillin/tazobactam and amoxicillin+temocillin for the rates of significant diarrhoea (34 versus 4 %, respectively; P < 0.0001) and for CDI (7 versus 0 %, respectively; P < 0.0028). This preliminary study suggests that the combination amoxicillin+temocillin is a viable alternative to piperacillin/tazobactam for the treatment of severe hospital-acquired pneumonia. This combination appears to be associated with fewer gastrointestinal adverse events. Further studies are needed to evaluate the place of amoxicillin+temocillin as empiric treatment of severe hospital-acquired pneumonia.
萨里郡一家大型急性医院服务提供商做出了一项处方决定,用阿莫西林+替莫西林替代哌拉西林/他唑巴坦,用于严重医院获得性肺炎的经验性治疗。做出这一决定是因为使用广谱β-内酰胺抗生素是艰难梭菌感染(CDI)和耐药性选择的已知风险因素。抗生素处方更改后,进行了一项回顾性审计,以评估这一变化的效果。回顾性分析了2011年1月至2012年7月因严重医院获得性肺炎住院并接受哌拉西林/他唑巴坦或阿莫西林+替莫西林经验性治疗的患者数据。分析了患者的临床特征、与肺炎发作相关的数据、临床疗效以及严重腹泻和CDI的发生率。从医院记录中识别出188例患者的192例严重医院获得性肺炎发作。98例患者接受了哌拉西林/他唑巴坦治疗,94例接受了阿莫西林+替莫西林治疗。在基线时,两个治疗组具有可比性,只是更多肾功能不全患者接受了哌拉西林/他唑巴坦治疗。临床疗效相当(分别为80%和82%;P = 0.86),但在严重腹泻发生率(分别为34%和4%;P < 0.0001)和CDI发生率(分别为7%和0%;P < 0.0028)方面,哌拉西林/他唑巴坦与阿莫西林+替莫西林之间存在差异。这项初步研究表明,阿莫西林+替莫西林组合是治疗严重医院获得性肺炎的哌拉西林/他唑巴坦的可行替代方案。这种组合似乎与较少的胃肠道不良事件相关。需要进一步研究来评估阿莫西林+替莫西林作为严重医院获得性肺炎经验性治疗的地位。