Steeden Jennifer A, Pandya Bejal, Tann Oliver, Muthurangu Vivek
UCL Centre for Cardiovascular Imaging, University College London, 30 Guildford Street, London, WC1N 1EH, UK.
The Heart Hospital, University College London Hospital Foundation Trust, London, W1G 8PH, UK.
J Cardiovasc Magn Reson. 2015 May 22;17(1):38. doi: 10.1186/s12968-015-0138-9.
Contrast enhanced magnetic resonance angiography (MRA) is generally performed during a long breath-hold (BH), limiting its utility in infants and small children. This study proposes a free-breathing (FB) time resolved MRA (TRA) technique for use in pediatric and adult congenital heart disease (CHD).
A TRA sequence was developed by combining spiral trajectories with sensitivity encoding (SENSE, x4 kx-ky and x2 kz) and partial Fourier (75% in kz). As no temporal data sharing is used, an independent 3D data set was acquired every 1.3s, with acceptable spatial resolution (2.3x2.3x2.3 mm). The technique was tested during FB over 50 consecutive volumes. Conventional BH-MRA and FB-TRA data was acquired in 45 adults and children with CHD. We calculated quantitative image quality for both sequences. Diagnostic accuracy was assessed in all patients from both sequences. Additionally, vessel measurements were made at the sinotubular junction (N = 43), proximal descending aorta (N = 43), descending aorta at the level of the diaphragm (N = 43), main pulmonary artery (N = 35), left pulmonary artery (N = 35) and the right pulmonary artery (N = 35). Intra and inter observer variability was assessed in a subset of 10 patients.
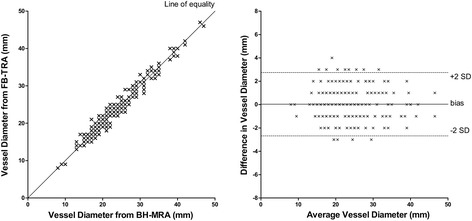
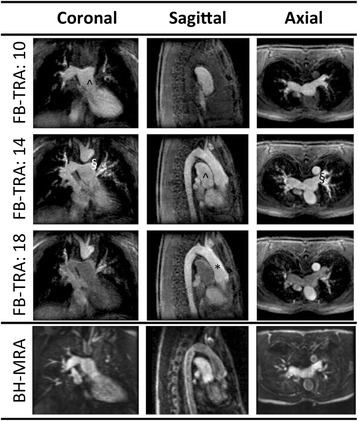
BH-MRA had significantly higher homogeneity in non-contrast enhancing tissue (coefficient of variance, P <0.0001), signal-to-noise ratio (P <0.0001), contrast-to-noise ratio (P <0.0001) and relative contrast (P = 0.02) compared to the FB-TRA images. However, homogeneity in the vessels was similar in both techniques (P = 0.52) and edge sharpness was significantly (P <0.0001) higher in FB-TRA compared to BH-MRA. BH-MRA provided overall diagnostic accuracy of 82%, and FB-TRA of 87%, with no statistical difference between the two sequences (P = 0.77). Vessel diameter measurements showed excellent agreement between the two techniques (r = 0.98, P <0.05), with no bias (0.0 mm, P = 0.71), and clinically acceptable limits of agreement (-2.7 to +2.8 mm). Inter and intra observer reproducibility showed good agreement of vessel diameters (r>0.988, P<0.0001), with negligible biases (between -0.2 and +0.1mm) and small limits of agreement (between -2.4 and +2.5mm).
We have described a FB-TRA technique that is shown to enable accurate diagnosis and vessel measures compared to conventional BH-MRA. This simplifies the MRA technique and will enable angiography to be performed in children and adults whom find breath-holding difficult.
对比增强磁共振血管造影(MRA)通常在长时间屏气(BH)期间进行,限制了其在婴儿和幼儿中的应用。本研究提出一种自由呼吸(FB)时间分辨MRA(TRA)技术,用于儿科和成人先天性心脏病(CHD)。
通过将螺旋轨迹与灵敏度编码(SENSE,x4 kx - ky和x2 kz)以及部分傅里叶(kz中75%)相结合,开发了一种TRA序列。由于未使用时间数据共享,每1.3秒获取一个独立的3D数据集,具有可接受的空间分辨率(2.3x2.3x2.3毫米)。该技术在FB期间连续采集50个容积进行测试。对45例患有CHD的成人和儿童进行了传统BH - MRA和FB - TRA数据采集。我们计算了两种序列的定量图像质量。评估了所有患者两种序列的诊断准确性。此外,在窦管交界处(N = 43)、近端降主动脉(N = 43)、膈肌水平的降主动脉(N = 4,3)、主肺动脉(N = 35)、左肺动脉(N = 35)和右肺动脉(N = 35)进行血管测量。在10例患者的子集中评估了观察者内和观察者间的变异性。
与FB - TRA图像相比,BH - MRA在非对比增强组织中的均匀性显著更高(变异系数,P < 0.0001)、信噪比(P < 0.0001)、对比噪声比(P < 0.0001)和相对对比度(P = 0.02)。然而,两种技术在血管中的均匀性相似(P = 0.52),并且与BH - MRA相比,FB - TRA的边缘清晰度显著更高(P < 0.0001)。BH - MRA的总体诊断准确性为82%,FB - TRA为87%,两种序列之间无统计学差异(P = 0.77)。血管直径测量显示两种技术之间具有极好的一致性(r = 0.98,P < 0.05),无偏差(0.0毫米,P = 0.71),并且一致性的临床可接受范围为(-2.7至+2.8毫米)。观察者间和观察者内的再现性显示血管直径具有良好的一致性(r > 0.988,P < 0.0001),偏差可忽略不计(-0.2至+0.1毫米之间),一致性范围较小(-2.4至+2.5毫米之间)。
我们描述了一种FB - TRA技术,与传统BH - MRA相比,该技术能够实现准确的诊断和血管测量。这简化了MRA技术,并将使血管造影能够在难以屏气的儿童和成人中进行。