Klaver Charlotte E L, Musters Gijsbert D, Bemelman Willem A, Punt Cornelis J A, Verwaal Victor J, Dijkgraaf Marcel G W, Aalbers Arend G J, van der Bilt Jarmila D W, Boerma Djamila, Bremers Andre J A, Burger Jacobus W A, Buskens Christianne J, Evers Pauline, van Ginkel Robert J, van Grevenstein Wilhelmina M U, Hemmer Patrick H J, de Hingh Ignace H J T, Lammers Laureen A, van Leeuwen Barbara L, Meijerink Wilhelmus J H J, Nienhuijs Simon W, Pon Jolien, Radema Sandra A, van Ramshorst Bert, Snaebjornsson Petur, Tuynman Jurriaan B, Te Velde Elisabeth A, Wiezer Marinus J, de Wilt Johannes H W, Tanis Pieter J
Department of surgery, Academic Medical Centre, University of Amsterdam, Post box 22660, 1105AZ, Amsterdam, The Netherlands.
Department of oncology, Academic Medical Centre, University of Amsterdam, Post box 22660, Amsterdam, The Netherlands.
BMC Cancer. 2015 May 24;15:428. doi: 10.1186/s12885-015-1430-7.
The peritoneum is the second most common site of recurrence in colorectal cancer. Early detection of peritoneal carcinomatosis (PC) by imaging is difficult. Patients eventually presenting with clinically apparent PC have a poor prognosis. Median survival is only about five months if untreated and the benefit of palliative systemic chemotherapy is limited. Only a quarter of patients are eligible for curative treatment, consisting of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CR/HIPEC). However, the effectiveness depends highly on the extent of disease and the treatment is associated with a considerable complication rate. These clinical problems underline the need for effective adjuvant therapy in high-risk patients to minimize the risk of outgrowth of peritoneal micro metastases. Adjuvant hyperthermic intraperitoneal chemotherapy (HIPEC) seems to be suitable for this purpose. Without the need for cytoreductive surgery, adjuvant HIPEC can be performed with a low complication rate and short hospital stay.
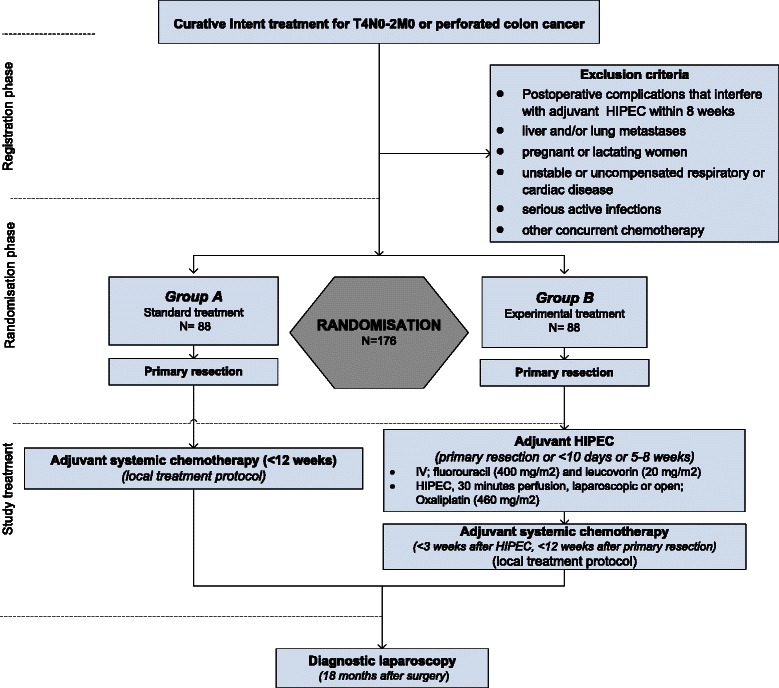
METHODS/DESIGN: The aim of this study is to determine the effectiveness of adjuvant HIPEC in preventing the development of PC in patients with colon cancer at high risk of peritoneal recurrence. This study will be performed in the nine Dutch HIPEC centres, starting in April 2015. Eligible for inclusion are patients who underwent curative resection for T4 or intra-abdominally perforated cM0 stage colon cancer. After resection of the primary tumour, 176 patients will be randomized to adjuvant HIPEC followed by routine adjuvant systemic chemotherapy in the experimental arm, or to systemic chemotherapy only in the control arm. Adjuvant HIPEC will be performed simultaneously or shortly after the primary resection. Oxaliplatin will be used as chemotherapeutic agent, for 30 min at 42-43 °C. Just before HIPEC, 5-fluorouracil and leucovorin will be administered intravenously. Primary endpoint is peritoneal disease-free survival at 18 months. Diagnostic laparoscopy will be performed routinely after 18 months postoperatively in both arms of the study in patients without evidence of disease based on routine follow-up using CT imaging and CEA.
Adjuvant HIPEC is assumed to reduce the expected 25 % absolute risk of PC in patients with T4 or perforated colon cancer to a risk of 10 %. This reduction is likely to translate into a prolonged overall survival.
NCT02231086 (Clinicaltrials.gov).
腹膜是结直肠癌复发的第二常见部位。通过影像学早期检测腹膜癌转移(PC)很困难。最终出现临床明显PC的患者预后较差。如果不治疗,中位生存期仅约五个月,姑息性全身化疗的益处有限。只有四分之一的患者有资格接受根治性治疗,包括细胞减灭术和热灌注腹腔内化疗(CR/HIPEC)。然而,其有效性高度依赖于疾病范围,且该治疗伴有相当高的并发症发生率。这些临床问题凸显了对高危患者进行有效辅助治疗以将腹膜微转移灶生长风险降至最低的必要性。辅助性热灌注腹腔内化疗(HIPEC)似乎适合此目的。无需进行细胞减灭术,辅助性HIPEC可在低并发症发生率和短住院时间的情况下进行。
方法/设计:本研究的目的是确定辅助性HIPEC在预防腹膜复发高危结肠癌患者发生PC方面的有效性。本研究将于2015年4月起在荷兰的九个HIPEC中心进行。符合纳入标准的是接受了T4期或腹腔内穿孔的cM0期结肠癌根治性切除术的患者。在切除原发肿瘤后,176名患者将被随机分为试验组,接受辅助性HIPEC,随后进行常规辅助性全身化疗;或分为对照组,仅接受全身化疗。辅助性HIPEC将在原发切除术后同时或不久后进行。将使用奥沙利铂作为化疗药物,在42 - 43°C下持续30分钟。就在HIPEC前,将静脉注射5-氟尿嘧啶和亚叶酸钙。主要终点是18个月时的腹膜无病生存期。在研究的两个组中,对于术后18个月时基于CT成像和癌胚抗原(CEA)的常规随访未发现疾病证据的患者,将常规进行诊断性腹腔镜检查。
辅助性HIPEC被认为可将T4期或穿孔性结肠癌患者预期的25%的PC绝对风险降低至10%的风险。这种降低可能会转化为总体生存期的延长。
NCT02231086(Clinicaltrials.gov)。