Unit of Oncologic and Pancreatic Surgery, Hospital University Reina Sofía, Menendez Pidal Av, 14004, Córdoba, Spain.
CIBERehd, IMIBIC, Hospital University Reina Sofía, Cordoba, Spain.
BMC Cancer. 2018 Feb 13;18(1):183. doi: 10.1186/s12885-018-4096-0.
Local relapse and peritoneal carcinomatosis (PC) for pT4 colon cancer is estimated in 15,6% and 36,7% for 12 months and 36 months from surgical resection respectively, achieving a 5 years overall survival of 6%. There are promising results using prophylactic HIPEC in this group of patients, and it is estimated that up to 26% of all T4 colon cancer could benefit from this treatment with a minimal morbidity. Adjuvant HIPEC is effective to avoid the possibility of peritoneal seeding after surgical resection. Taking into account these results and the cumulative experience in HIPEC use, we will lead a randomized controlled trial to determine the effectiveness and safety of adjuvant treatment with HIPEC vs. standard treatment in patients with colon cancer at high risk of peritoneal recurrence (pT4).
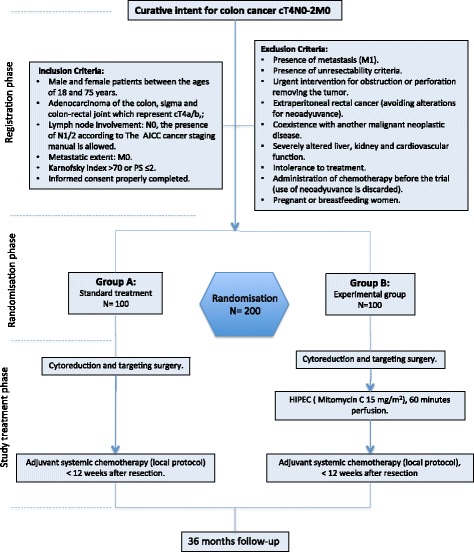
METHODS/DESIGN: The aim of this study is to determine the effectiveness and safety of adjuvant HIPEC in preventing the development of PC in patients with colon cancer with a high risk of peritoneal recurrence (cT4). This study will be carried out in 15 Spanish HIPEC centres. Eligible for inclusion are patients who underwent curative resection for cT4NxM0 stage colon cancer. After resection of the primary tumour, 200 patients will be randomized to adjuvant HIPEC followed by routine adjuvant systemic chemotherapy in the experimental arm, or to systemic chemotherapy only in the control arm. Adjuvant HIPEC will be performed simultaneously after the primary resection. Mitomycin C will be used as chemotherapeutic agent, for 60 min at 42-43 °C. Primary endpoint is loco-regional control (LC) in months and the rate of loco-regional control (%LC) at 12 months and 36 months after resection.
We assumed that adjuvant HIPEC will reduce the expected absolute risk of peritoneal recurrence from 36% to 18% at 36 months for T4 colon-rectal carcinoma.
NCT02614534 ( clinicaltrial.gov ) Nov-2015.
局部复发和腹膜癌转移(PC)对于 pT4 结肠癌,分别在手术后 12 个月和 36 个月时的预估发生率为 15.6%和 36.7%,5 年总生存率为 6%。对于这组患者,采用预防性 HIPEC 治疗有很好的效果,据估计,多达 26%的所有 T4 结肠癌患者可能从这种治疗中获益,而且发病率极低。辅助 HIPEC 对于避免手术后发生腹膜种植有效果。考虑到这些结果和 HIPEC 使用的累积经验,我们将进行一项随机对照试验,以确定辅助 HIPEC 治疗与标准治疗在腹膜复发高风险(pT4)的结肠癌患者中的有效性和安全性。
方法/设计:本研究的目的是确定辅助 HIPEC 在预防腹膜复发高风险(cT4)的结肠癌患者中发生 PC 的有效性和安全性。这项研究将在 15 个西班牙 HIPEC 中心进行。纳入标准为接受根治性切除的 cT4NxM0 期结肠癌患者。原发性肿瘤切除后,将 200 名患者随机分为实验组接受辅助 HIPEC 联合常规辅助全身化疗,对照组仅接受全身化疗。辅助 HIPEC 将在原发性肿瘤切除后同时进行。顺铂作为化疗药物,在 42-43°C 下使用 60 分钟。主要终点是术后 12 个月和 36 个月的局部区域控制(LC)和局部区域控制率(%LC)。
我们假设辅助 HIPEC 将使 T4 结肠直肠癌术后 36 个月时腹膜复发的预期绝对风险从 36%降低到 18%。
NCT02614534(clinicaltrial.gov),2015 年 11 月。