Hoole Stephen P, Jaworski Catherine, Brown Adam J, McCormick Liam M, Agrawal Bobby, Clarke Sarah C, West Nick E J
Department of Interventional Cardiology , Papworth Hospital , Cambridge , UK.
Department of Radiology , Papworth Hospital , Cambridge , UK.
Open Heart. 2015 May 16;2(1):e000238. doi: 10.1136/openhrt-2015-000238. eCollection 2015.
Utilising a novel study design, we evaluated serial measurements of the index of microcirculatory resistance (IMR) in patients undergoing primary percutaneous coronary intervention (PPCI) for ST-segment elevation myocardial infarction (STEMI) to assess the impact of device therapy on microvascular function, and determine what proportion of microvascular injury is related to the PPCI procedure, and what is an inevitable consequence of STEMI.
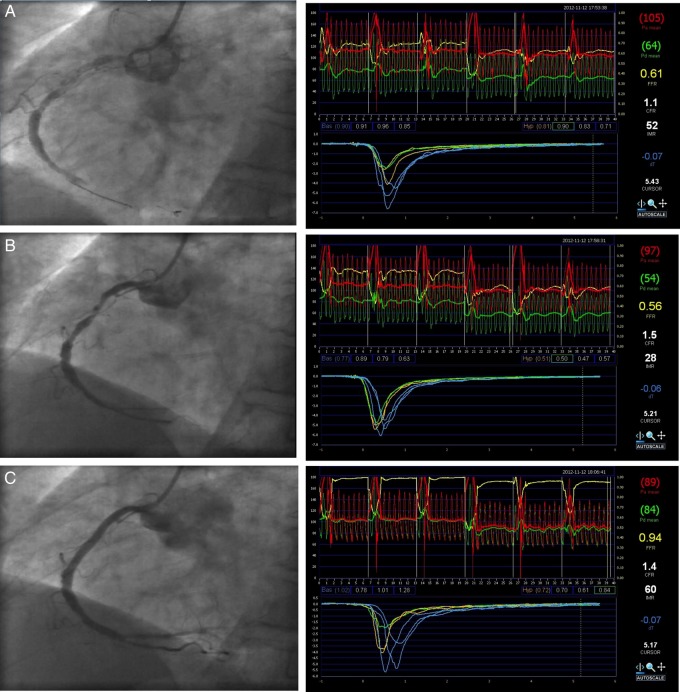
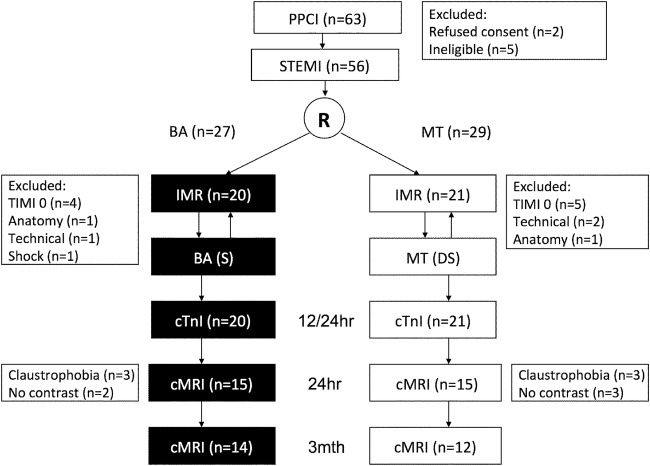
41 patients undergoing PPCI for STEMI were randomised to balloon angioplasty (BA, n=20) or manual thrombectomy (MT, n=21) prior to stenting. Serial IMR measurements, corrected for collaterals, were recorded at baseline and at each stage of the procedure. Microvascular obstruction (MVO) and infarct size at 24 h and 3 months were measured by troponin and cardiac MRI (CMR).
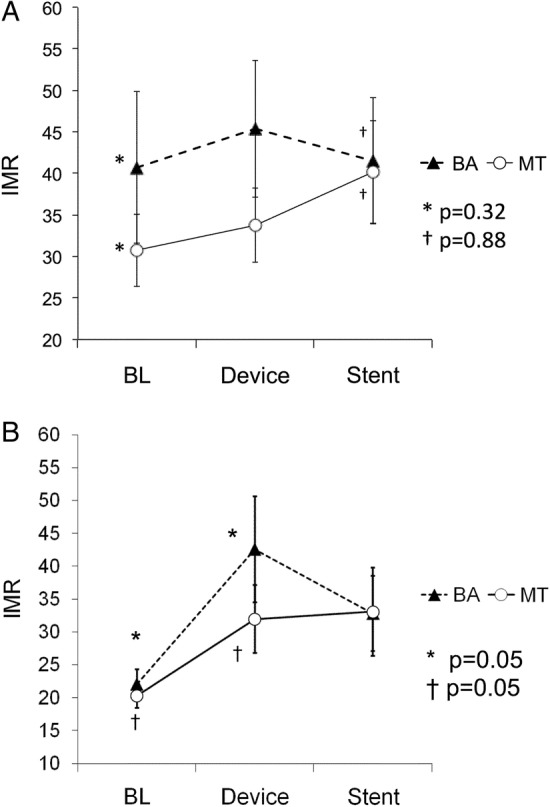
IMR did not change significantly following PPCI, but patients with lower IMR values (<32, n=30) at baseline had a significant increase in IMR following PPCI (baseline: 21.2±7.9 vs post-stent: 33.0±23.7, p=0.01) attributable to prestent IRA instrumentation (baseline: 21.7±8.0 vs post-BA or MT: 36.9±25.9, p=0.006). Post-stent IMR correlated with early MVO on CMR (p=0.01). There was no significant difference in post-stent IMR, presence of early MVO or final infarct size between patients with BA and patients treated with MT.
Patients with STEMI and less microcirculatory dysfunction may be susceptible to acute iatrogenic microcirculatory injury from prestent coronary devices. MT did not appear to be superior to BA in maintaining microcirculatory integrity when the guide wire partially restores IRA flow during PPCI.
ISRCTN31767278.
采用一种新颖的研究设计,我们评估了接受ST段抬高型心肌梗死(STEMI)直接经皮冠状动脉介入治疗(PPCI)患者的微循环阻力指数(IMR)的系列测量值,以评估器械治疗对微血管功能的影响,并确定微血管损伤的比例中哪些与PPCI手术相关,哪些是STEMI的必然结果。
41例接受STEMI的PPCI患者在支架置入术前被随机分为球囊血管成形术(BA,n = 20)或手动血栓切除术(MT,n = 21)。记录基线时以及手术各阶段经侧支循环校正后的IMR系列测量值。通过肌钙蛋白和心脏磁共振成像(CMR)测量24小时和3个月时的微血管阻塞(MVO)和梗死面积。
PPCI后IMR无显著变化,但基线时IMR值较低(<32,n = 30)的患者在PPCI后IMR显著增加(基线:21.2±7.9 vs 支架置入后:33.0±23.7,p = 0.01),这归因于支架置入前梗死相关动脉(IRA)的器械操作(基线:21.7±8.0 vs BA或MT后:36.9±25.9,p = 0.006)。支架置入后IMR与CMR上的早期MVO相关(p = 0.01)。BA患者和接受MT治疗的患者在支架置入后IMR、早期MVO的存在或最终梗死面积方面无显著差异。
STEMI且微循环功能障碍较轻的患者可能易受支架置入前冠状动脉器械导致的急性医源性微循环损伤影响。当导丝在PPCI期间部分恢复IRA血流时,MT在维持微循环完整性方面似乎并不优于BA。
ISRCTN31767278。