Papierska Lucyna, Ćwikła Jarosław, Rabijewski Michał, Glinicki Piotr, Otto Maciej, Kasperlik-Załuska Anna
Department of Endocrinology, Medical Center of Postgraduate Education, CMKP, ul. Marymoncka 99, 01-809, Warsaw, Poland.
Department of Internal Diseases, Metabolism and Endocrinology, Bielański Hospital, Szpital Bielański, ul. Cegłowska 80, 01-809, Warsaw, Poland.
Abdom Imaging. 2015 Oct;40(7):2453-60. doi: 10.1007/s00261-015-0452-6.
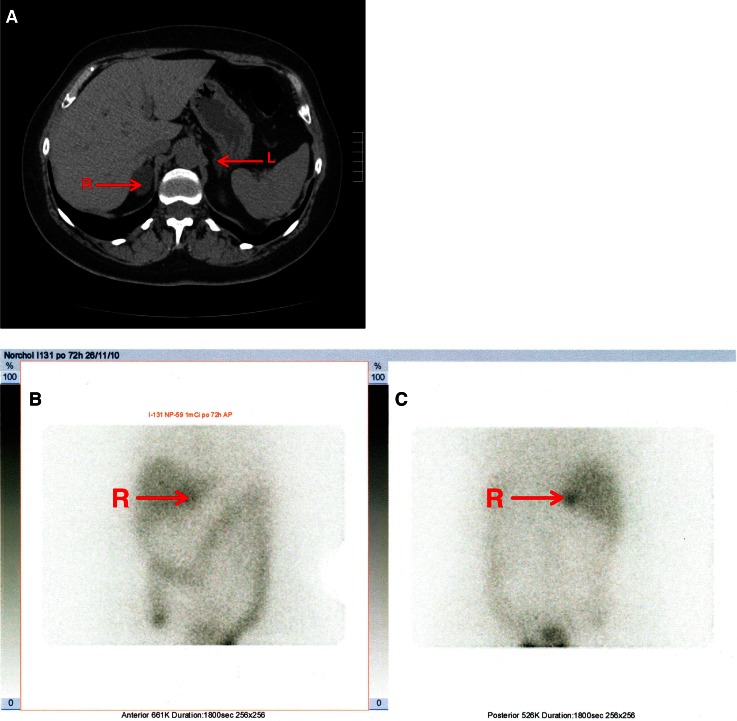
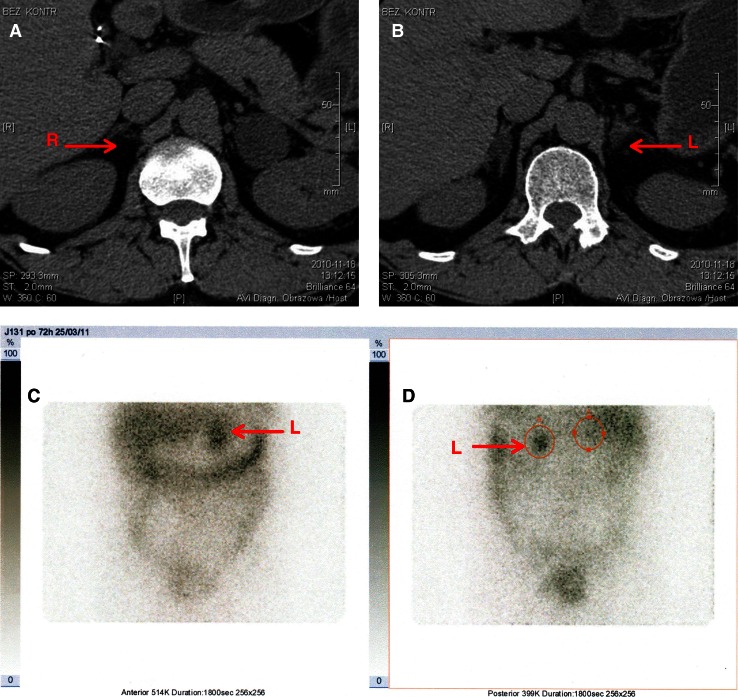
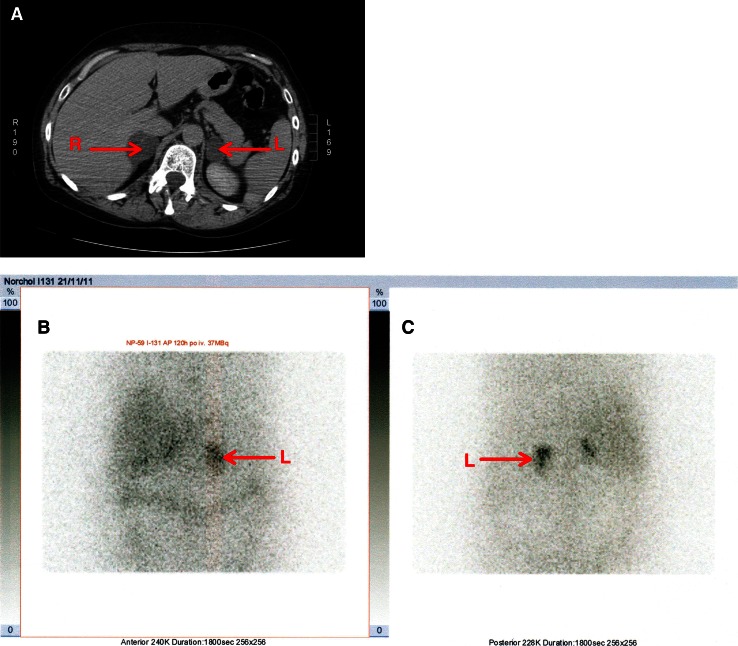
Adrenal scintigraphy with 131I-6β-iodomethylnorcholesterol is considered by several authors the gold standard for assessing tumors with subclinical hypercortisolemia. However, most of the described series consist mainly of cases with unilateral lesions. The aim of our study was to assess whether scintigraphy is useful in choosing the adrenalectomy side in the case of bilateral adrenal tumors with subclinical hypercortisolemia.
The study focused on 15 consecutive patients with benign bilateral adrenal tumors and subclinical hypercortisolemia. The scintigraphy with 131I-6β-iodomethylnorcholesterol was performed. Fourteen patients underwent unilateral adrenalectomy; the gland with predominant uptake on scintigraphy was removed. Cortisol and ACTH concentrations were measured one and six months after surgery. Post-dexamethasone cortisolemia was assessed six months after surgery. To date, the patients have been under postoperative observation for 1-4 years.
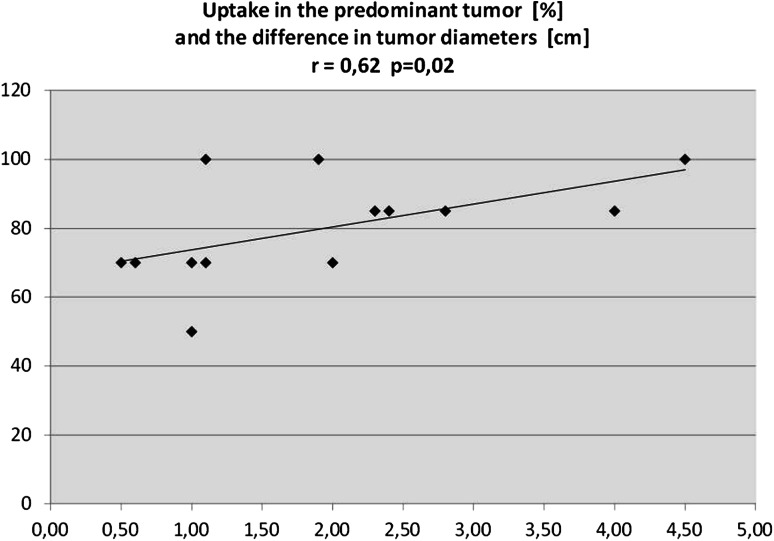
Four patients showed unilateral uptake of radiotracer, and nine patients showed predominant accumulation of radiotracer in one of the adrenal glands. The smaller tumor was predominant in 2 cases. Percentage of activity on the predominant side correlates positively with the difference between tumors' diameters. Unilateral uptake of radiotracer predicts long-lasting postoperative insufficiency of the second adrenal gland. Excision of predominating tumor led to cessation of hypercortisolemia in all patients.
The corticoadrenal scintigraphy is useful in choosing the side for operation in the case of bilateral adrenal tumors with subclinical hypercortisolemia.
多位作者认为,用131I-6β-碘甲基去甲胆固醇进行肾上腺闪烁扫描是评估亚临床皮质醇增多症肿瘤的金标准。然而,大多数已报道的系列病例主要为单侧病变。我们研究的目的是评估闪烁扫描在选择对侧肾上腺切除术治疗双侧肾上腺肿瘤合并亚临床皮质醇增多症时是否有用。
本研究聚焦于15例连续的双侧肾上腺良性肿瘤合并亚临床皮质醇增多症患者。进行了131I-6β-碘甲基去甲胆固醇闪烁扫描。14例患者接受了单侧肾上腺切除术;切除闪烁扫描时摄取量占优势的腺体。在术后1个月和6个月测量皮质醇和促肾上腺皮质激素(ACTH)浓度。在术后6个月评估地塞米松后血皮质醇水平。迄今为止,患者已接受术后观察1至4年。
4例患者显示放射性示踪剂单侧摄取,9例患者显示放射性示踪剂在一侧肾上腺中主要积聚。2例患者中较小的肿瘤占优势。优势侧的活性百分比与肿瘤直径之差呈正相关。放射性示踪剂的单侧摄取预示着对侧肾上腺术后长期功能不全。切除占优势的肿瘤导致所有患者的皮质醇增多症停止。
在双侧肾上腺肿瘤合并亚临床皮质醇增多症的情况下,肾上腺皮质闪烁扫描有助于选择手术侧。