Cuzick J, Stone S, Fisher G, Yang Z H, North B V, Berney D M, Beltran L, Greenberg D, Møller H, Reid J E, Gutin A, Lanchbury J S, Brawer M, Scardino P
Centre for Cancer Prevention, Wolfson Institute of Preventive Medicine, Queen Mary University of London, London, UK.
Myriad Genetics, Inc., Salt Lake City, UT, USA.
Br J Cancer. 2015 Jul 28;113(3):382-9. doi: 10.1038/bjc.2015.223. Epub 2015 Jun 23.
The natural history of prostate cancer is highly variable and difficult to predict accurately. Better markers are needed to guide management and avoid unnecessary treatment. In this study, we validate the prognostic value of a cell cycle progression score (CCP score) independently and in a prespecified linear combination with standard clinical variables, that is, a clinical-cell-cycle-risk (CCR) score.
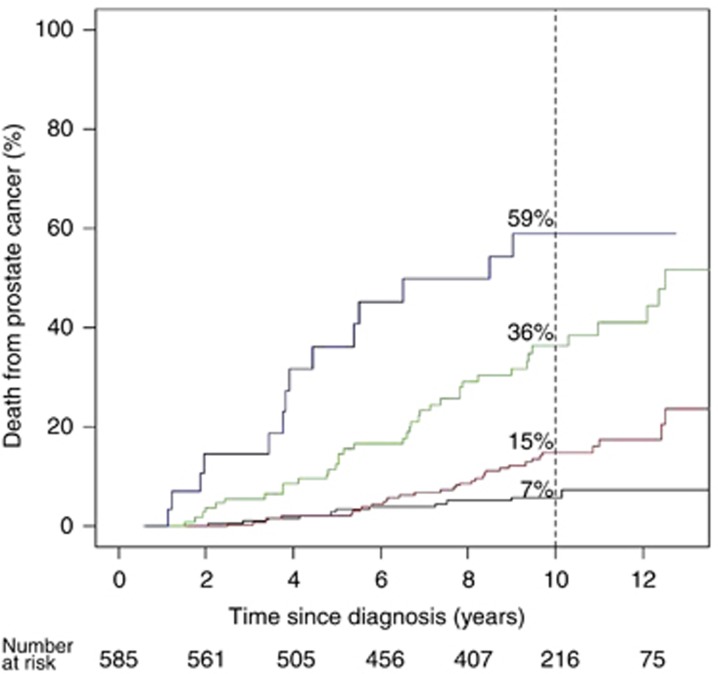
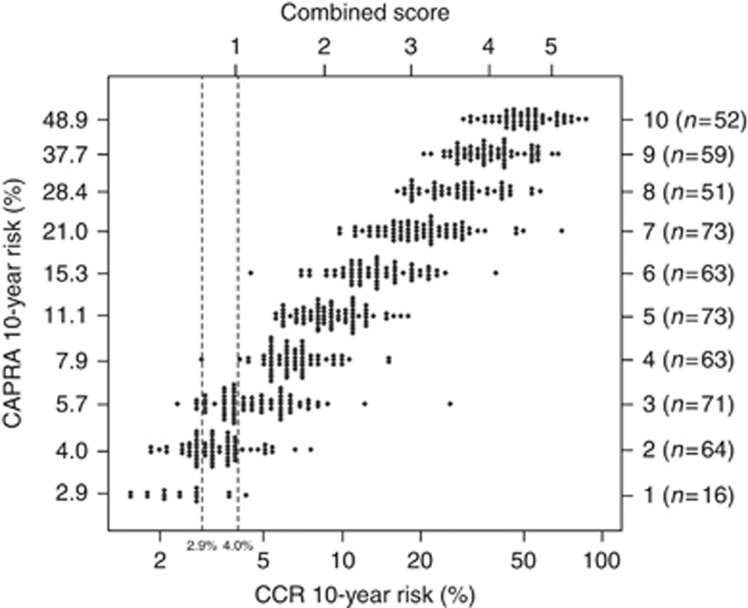
Paraffin sections from 761 men with clinically localized prostate cancer diagnosed by needle biopsy and managed conservatively in the United Kingdom, mostly between 2000 and 2003. The primary end point was prostate cancer death. Clinical variables consisted of centrally reviewed Gleason score, baseline PSA level, age, clinical stage, and extent of disease; these were combined into a single predefined risk assessment (CAPRA) score. Full data were available for 585 men who formed a fully independent validation cohort.
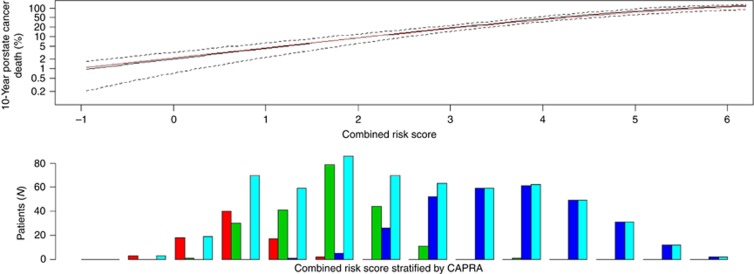
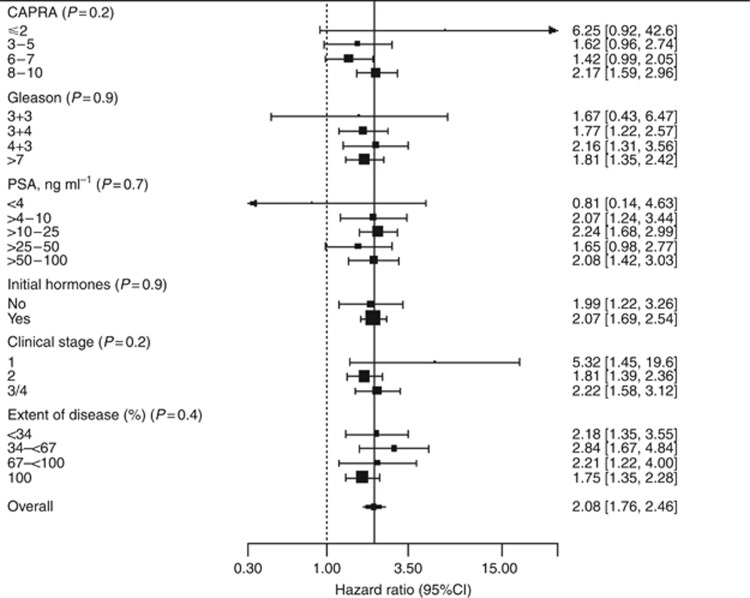
In univariate analysis, the CCP score hazard ratio was 2.08 (95% CI (1.76, 2.46), P<10(-13)) for one unit change of the score. In multivariate analysis including CAPRA, the CCP score hazard ratio was 1.76 (95% CI (1.44, 2.14), P<10(-6)). The predefined CCR score was highly predictive, hazard ratio 2.17 (95% CI (1.83, 2.57), χ(2)=89.0, P<10(-20)) and captured virtually all available prognostic information.
The CCP score provides significant pretreatment prognostic information that cannot be provided by clinical variables and is useful for determining which patients can be safely managed conservatively, avoiding radical treatment.
前列腺癌的自然病程高度可变,难以准确预测。需要更好的标志物来指导治疗管理并避免不必要的治疗。在本研究中,我们独立验证了细胞周期进展评分(CCP评分)的预后价值,并将其与标准临床变量进行预先设定的线性组合,即临床 - 细胞周期风险(CCR)评分。
对761名经针吸活检诊断为临床局限性前列腺癌且在英国接受保守治疗的男性患者的石蜡切片进行研究,这些患者大多在2000年至2003年期间。主要终点是前列腺癌死亡。临床变量包括经中心审核的 Gleason评分、基线PSA水平、年龄、临床分期和疾病范围;这些被合并为一个单一的预定义风险评估(CAPRA)评分。585名男性患者有完整数据,他们构成了一个完全独立的验证队列。
在单变量分析中,CCP评分每变化一个单位,风险比为2.08(95%可信区间(1.76, 2.46),P < 10⁻¹³)。在包括CAPRA的多变量分析中,CCP评分风险比为1.76(95%可信区间(1.44, 2.14),P < 10⁻⁶)。预定义的CCR评分具有高度预测性,风险比为2.17(95%可信区间(1.83, 2.57),χ² = 89.0,P < 10⁻²⁰),并且几乎捕捉了所有可用的预后信息。
CCP评分提供了临床变量无法提供的重要治疗前预后信息,有助于确定哪些患者可以安全地接受保守治疗,避免根治性治疗。