McDaniel Anna M, Vickerman Katrina A, Stump Timothy E, Monahan Patrick O, Fellows Jeffrey L, Weaver Michael T, Carlini Beatriz H, Champion Victoria L, Zbikowski Susan M
College of Nursing, University of Florida, Gainesville, Florida, USA.
Alere Wellbeing, Seattle, Washington, USA.
BMJ Open. 2015 Jun 29;5(6):e007260. doi: 10.1136/bmjopen-2014-007260.
To test adding an interactive voice response (IVR)-supported protocol to standard quitline treatment to prevent relapse among recently quit smokers.
Parallel randomised controlled trial with three arms: standard quitline, standard plus technology enhanced quitline with 10 risk assessments (TEQ-10), standard plus 20 TEQ assessments (TEQ-20).
Quit For Life (QFL) programme.
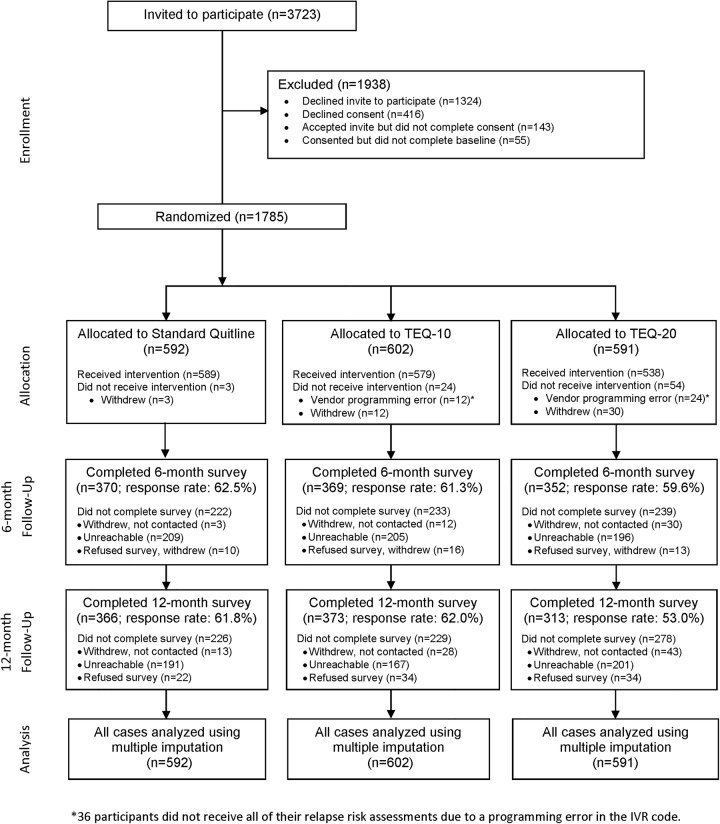
1785 QFL enrolees through 19 employers or health plans who were 24+ h quit.
QFL is a 5-call telephone-based cessation programme including medications and web-based support. TEQ interventions included 10 or 20 IVR-delivered relapse risk assessments over 8 weeks with automated transfer to counselling for those at risk.
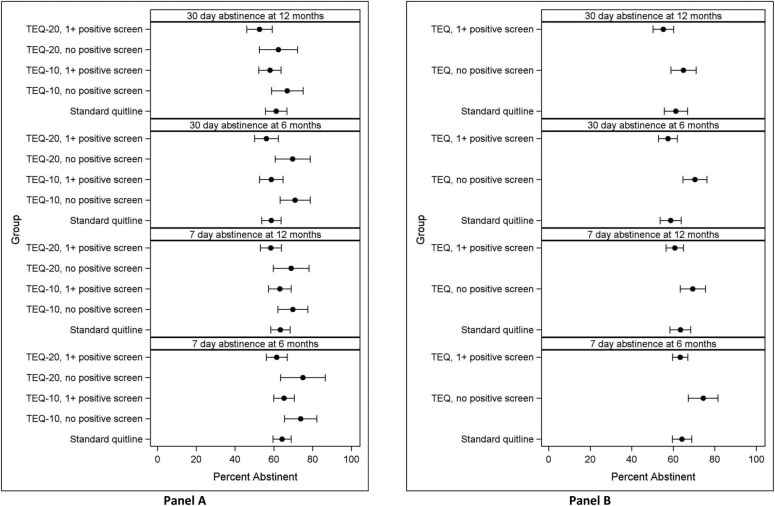
Self-reported 7-day and 30-day abstinence assessed at 6-month and 12-month post-enrolment (response rates: 61% and 59%, respectively). Missing data were imputed.
1785 were randomised (standard n=592, TEQ-10 n=602, TEQ-20 n=591). Multiple imputation-derived, intent-to-treat 30-day quit rates (95% CI) at 6 months were 59.4% (53.7% to 63.8%) for standard, 62.3% (57.7% to 66.9%) for TEQ-10, 59.4% (53.7% to 65.1%) for TEQ-20 and 30-day quit rates at 12 months were 61.2% (55.6% to 66.8%) for standard, 60.6% (56.0% to 65.2%) for TEQ-10, 54.9% (49.0% to 60.9%) for TEQ-20. There were no significant differences in quit rates. 73.3% of TEQ participants were identified as at-risk by IVR assessments; on average, participants completed 0.41 IVR-transferred counselling calls. Positive risk assessments identified participants less likely (OR=0.56, 95% CI 0.42 to 0.76) to be abstinent at 6 months.
Standard treatment was highly effective, with 61% remaining abstinent at 12 months using multiple imputation intent-to-treat (intent-to-treat missing=smoking quit rate: 38%). TEQ assessments identified quitters at risk for relapse. However, adding IVR-transferred counselling did not yield higher quit rates. Research is needed to determine if alternative designs can improve outcomes.
NCT00888992.
测试在标准戒烟热线治疗中添加交互式语音应答(IVR)支持的方案,以防止近期戒烟者复发。
平行随机对照试验,分为三组:标准戒烟热线、标准加10次风险评估的技术增强戒烟热线(TEQ-10)、标准加20次TEQ评估(TEQ-20)。
终身戒烟(QFL)项目。
通过19个雇主或健康计划招募的1785名QFL参与者,他们已戒烟24小时以上。
QFL是一个基于电话的5次呼叫戒烟项目,包括药物治疗和基于网络的支持。TEQ干预措施包括在8周内通过IVR进行10次或20次复发风险评估,并将有风险的人自动转介到咨询服务。
在入组后6个月和12个月评估自我报告的7天和30天戒烟情况(应答率分别为61%和59%)。缺失数据进行了插补。
1785人被随机分组(标准组n=592,TEQ-10组n=602,TEQ-20组n=591)。多重插补得出的意向性分析6个月时的30天戒烟率(95%CI),标准组为59.4%(53.7%至63.8%),TEQ-10组为62.3%(57.7%至66.9%),TEQ-20组为59.4%(53.7%至65.1%);12个月时的30天戒烟率,标准组为61.2%(55.6%至66.8%),TEQ-10组为60.6%(56.0%至65.2%),TEQ-20组为54.9%(49.0%至60.9%)。戒烟率无显著差异。73.3%的TEQ参与者通过IVR评估被确定为有风险;平均而言,参与者完成了0.41次IVR转介的咨询电话。阳性风险评估表明参与者在6个月时戒烟的可能性较小(OR=0.56,95%CI 0.42至0.76)。
标准治疗非常有效,使用多重插补意向性分析,12个月时61%的人保持戒烟状态(意向性分析缺失=吸烟戒烟率:38%)。TEQ评估识别出有复发风险的戒烟者。然而,添加IVR转介的咨询并没有提高戒烟率。需要进行研究以确定替代设计是否能改善结局。
NCT00888992。