Barzenje Dlawer Abdulla, Cvancarova Småstuen Milada, Liestøl Knut, Fosså Alexander, Delabie Jan, Kolstad Arne, Holte Harald
Department of Oncology, Ostfold Hospital Trust, Fredrikstad, Norway.
Department of Biostatistics, Oslo University Hospital, Oslo, Norway.
PLoS One. 2015 Jul 6;10(7):e0131158. doi: 10.1371/journal.pone.0131158. eCollection 2015.
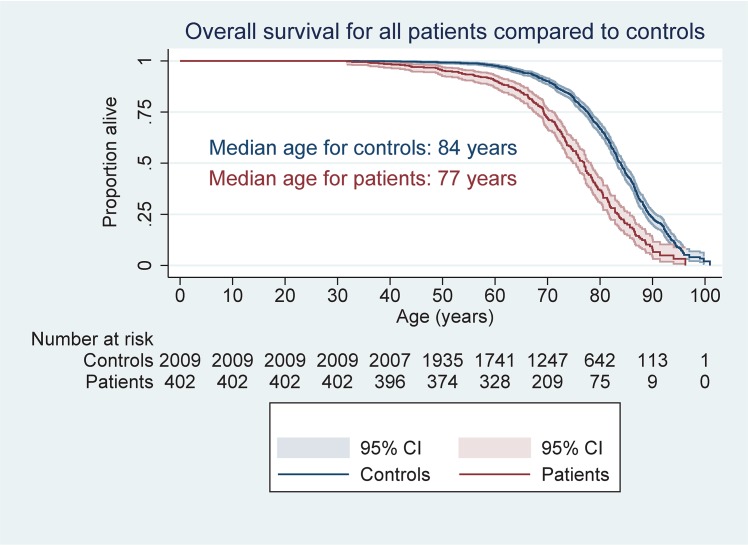
To investigate outcome for patients with follicular lymphoma (FL) stage I-II treated at a population-based referral institution with a median follow-up of 15 years. Overall and cause-specific survival was compared to that of a sex, age and residency matched individuals from normal population.
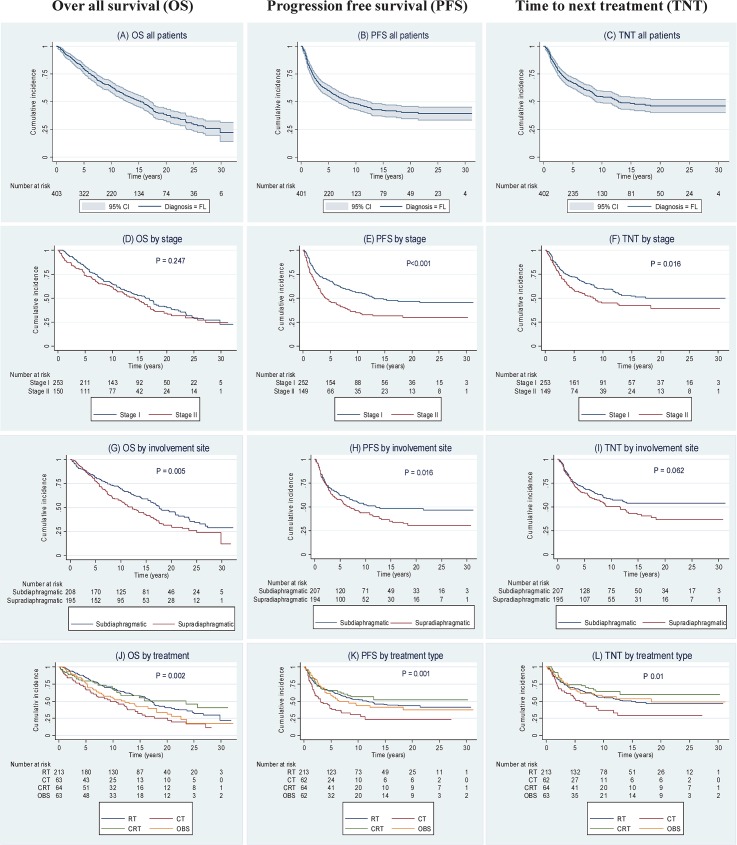
404 patients with early stage FL treated between 1980 and 2005 were retrospectively analyzed. Two of three patients had stage I disease. Based on clinical characteristics, first line treatments were radiotherapy (RT) (48% of patients), chemotherapy (CT) (16%), combined chemo-and radiotherapy (CRT) (16%) or observation (OBS) (15%). Survival was modeled with Kaplan-Meier methodology. Multivariate analyses were performed with the Cox model.
Fifteen years overall survival (OS), progression free survival (PFS) and time to next treatment (TNT) were 50% (95% confidence interval [CI]: 45-55), 42% (95% CI: 36-47) and 48% (95% CI, 42-54), respectively. For patients treated with RT 97% achieved a complete remission, and 15 year OS, PFS and TNT were 57% (95% CI, 50-64), 46% (95% CI, 39-54) and 49% (95% CI, 42-57), respectively. Relapse rate after RT and CRT was 49% and 36%, respectively. Only 2% of patients who received RT or CRT relapsed inside the radiation field and 5% had isolated near-field relapse. No statistical differences were found between treatment groups regarding death from cardiovascular disease or incidence of second cancer. Compared to a matched normal population, non-lymphoma cancer mortality was higher among patients given RT, hazard ratio 1.66 (95% CI: 1.14-2.42; P<0.01). Compared to other treatment modalities, patients selected for observation without treatment did not have inferior outcome.
A differentiated treatment strategy in early stage FL results in long term survival for the majority of patients. OBS is a valid initial choice for selected patients without lymphoma-related symptoms.
调查在一家基于人群的转诊机构接受治疗的 I-II 期滤泡性淋巴瘤(FL)患者的预后,中位随访时间为 15 年。将总生存率和病因特异性生存率与来自正常人群的性别、年龄和居住地匹配的个体进行比较。
回顾性分析了 1980 年至 2005 年间接受治疗的 404 例早期 FL 患者。三分之二的患者为 I 期疾病。根据临床特征,一线治疗方法为放疗(RT)(48%的患者)、化疗(CT)(16%)、放化疗联合(CRT)(16%)或观察(OBS)(15%)。采用 Kaplan-Meier 方法对生存率进行建模。使用 Cox 模型进行多变量分析。
15 年总生存率(OS)、无进展生存率(PFS)和下次治疗时间(TNT)分别为 50%(95%置信区间[CI]:45-55)、42%(95%CI:36-47)和 48%(95%CI,42-54)。接受 RT 治疗的患者中,97%实现了完全缓解,15 年 OS、PFS 和 TNT 分别为 57%(95%CI,50-64)、46%(95%CI,39-54)和 49%(95%CI,42-57)。RT 和 CRT 后的复发率分别为 49%和 36%。接受 RT 或 CRT 的患者中,仅 2%在放射野内复发,5%有孤立的近野复发。各治疗组在心血管疾病死亡或第二癌症发病率方面未发现统计学差异。与匹配的正常人群相比,接受 RT 的患者中非淋巴瘤癌症死亡率更高,风险比为 1.66(95%CI:1.14-2.42;P<0.01)。与其他治疗方式相比,选择观察而不进行治疗的患者预后并不差。
早期 FL 的差异化治疗策略可为大多数患者带来长期生存。对于无淋巴瘤相关症状的选定患者,OBS 是一种有效的初始选择。