Bekondi Claudine, Zanchi Roberta, Seck Abdoulaye, Garin Benoit, Giles-Vernick Tamara, Gody Jean Chrysotome, Bata Petulla, Pondy Angèle, Tetang Suzie Moyo, Ba Mamadou, Ekobo Chantal Same, Rousset Dominique, Sire Jean-Marie, Maylin Sarah, Chartier Loïc, Njouom Richard, Vray Muriel
Laboratoire des Virus Oncogènes, Institut Pasteur de Bangui, rue Pasteur, BP 923, Bangui, République Centrafricaine.
Unité d'Epidémiologie des Maladies Emergentes, Institut Pasteur, 25-28 rue du Docteur Roux, 75015, Paris, France.
BMC Infect Dis. 2015 Jul 12;15:267. doi: 10.1186/s12879-015-1000-2.
Hepatitis B is a major health concern in Africa. The vaccine against hepatitis B virus (HBV) was introduced into the Expanded Programme on Immunization (EPI) of Cameroon and Senegal in 2005, and of CAR (Central African Republic) in 2008. A cross-sectional study was conducted to assess HBV immunization coverage following the vaccine's introduction into the EPI and factors associated with having been vaccinated.
All hospitalized children, regardless of the reasons for their hospitalization, between 3 months and 6 years of age, for whom a blood test was scheduled during their stay and whose condition allowed for an additional 2 mL blood sample to be taken, and who provided the parent's written consent were included. All children anti-HBs- and anti-HBc + were tested for HBsAg. Vaccination coverage was assessed in three different ways: immunization card, maternal recall and serologic anti-HBs profile.
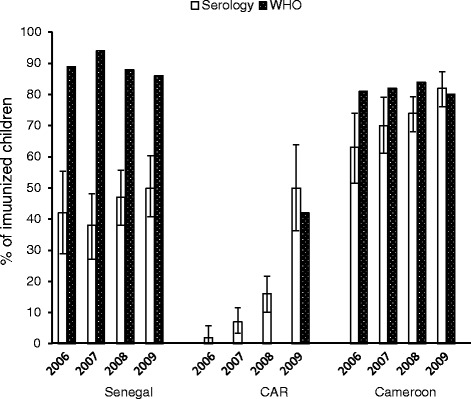
1783 children were enrolled between April 2009 and May 2010. An immunization card was only available for 24 % of the children. The median age was 21 months. Overall HBV immunization coverage based on immunization cards was 99 %, 49 % and 100 % in Cameroon, CAR and Senegal, respectively (p < 0,001). The immunization rate based on maternal recall was 91 %, 17 % and 88 % in Cameroon, CAR and Senegal, respectively (p < 0,001). According to serology (anti-HBs titer ≥ 10 mUI/mL and anti-HBc-), the coverage rate was 68 %, 13 % and 46 % in Cameroon, CAR and Senegal, respectively (p < 0,001). In Senegal and Cameroon, factors associated with having been vaccinated were: mother's higher education (OR = 2.2; 95 % CI [1.5-3.2]), no malnutrition (OR = 1.6; 95 % CI [1.1-2.2]), access to flushing toilets (OR = 1.6; 95 % CI [1.1-2.3]), and < 24 months old (OR = 2.1; 95 % CI [1.3-3.4] between 12 and 23 months and OR = 2.7; 95 % CI [1.6-4.4] < 12 months). The prevalence of HBV-infected children (HBsAg+) were 0.7 %, 5.1 %, and 0.2 % in Cameroon, CAR and Senegal, respectively (p < 0.001).
Assessing immunization coverage based on immunization cards, maternal recall or administrative data could be usefully reinforced by epidemiological data combined with immunological profiles. Serology-based studies should be implemented regularly in African countries, as recommended by the WHO. Malnutrition, lack of maternal education and poverty are factors associated with vaccine non-compliance. The countries' vaccination programs should actively address these problems.
乙型肝炎是非洲主要的健康问题。2005年,乙型肝炎病毒(HBV)疫苗被引入喀麦隆和塞内加尔的扩大免疫规划(EPI),2008年被引入中非共和国的扩大免疫规划。开展了一项横断面研究,以评估该疫苗引入EPI后的HBV免疫覆盖率以及与接种疫苗相关的因素。
纳入所有3个月至6岁的住院儿童,无论其住院原因如何,这些儿童在住院期间计划进行血液检查,且其病情允许额外采集2 mL血样,并获得了家长的书面同意。对所有抗-HBs-和抗-HBc+的儿童进行HBsAg检测。通过三种不同方式评估疫苗接种覆盖率:免疫卡、母亲回忆和血清学抗-HBs谱。
2009年4月至2010年5月期间共纳入1783名儿童。只有24%的儿童有免疫卡。中位年龄为21个月。基于免疫卡的总体HBV免疫覆盖率在喀麦隆、中非共和国和塞内加尔分别为99%、49%和100%(p<0.001)。基于母亲回忆的免疫接种率在喀麦隆、中非共和国和塞内加尔分别为91%、17%和88%(p<0.001)。根据血清学(抗-HBs滴度≥10 mUI/mL且抗-HBc-),喀麦隆、中非共和国和塞内加尔的覆盖率分别为68%、13%和46%(p<0.001)。在塞内加尔和喀麦隆,与接种疫苗相关的因素有:母亲受教育程度较高(OR=2.2;95%CI[1.5-3.2])、无营养不良(OR=1.6;95%CI[1.1-2.2])、使用冲水马桶(OR=1.6;95%CI[1.1-2.3])以及年龄<24个月(12至23个月时OR=2.1;95%CI[1.3-3.4],<12个月时OR=2.7;95%CI[1.6-4.4])。喀麦隆、中非共和国和塞内加尔HBV感染儿童(HBsAg+)的患病率分别为0.7%、5.1%和0.2%(p<0.001)。
结合免疫数据的流行病学数据可有效加强基于免疫卡、母亲回忆或行政数据的免疫覆盖率评估。应按照世界卫生组织的建议,定期在非洲国家开展基于血清学的研究。营养不良、母亲教育程度低和贫困是与疫苗接种不依从相关的因素。各国的疫苗接种计划应积极解决这些问题。