Duclos Martine, Dejager Sylvie, Postel-Vinay Nicolas, di Nicola Sylvie, Quéré Stéphane, Fiquet Béatrice
Department of Sport Medicine and Functional Explorations, University-Hospital (CHU), G Montpied Hospital; INRA, UNH, CRNH Auvergne, France ; Nutrition Department, University of Auvergne, Clermont-Ferrand, Auvergne, France.
Department of Endocrinology and Metabolism, La Pitié-Salpétrière Hospital, Paris, France ; Clinical and Scientific Affairs, Novartis Pharma SAS, Rueil-Malmaison, France.
Vasc Health Risk Manag. 2015 Jun 29;11:361-71. doi: 10.2147/VHRM.S84832. eCollection 2015.
Although physical activity (PA) is key in the management of type 2 diabetes (T2DM) and hypertension, it is difficult to implement in practice.
Cross-sectional, observational study. Participating physicians were asked to recruit two active and four inactive patients, screened with the Ricci-Gagnon (RG) self-questionnaire (active if score ≥16). Patients subsequently completed the International Physical Activity Questionnaire. The objective was to assess the achievement of individualized glycated hemoglobin and blood pressure goals (<140/90 mmHg) in the active vs inactive cohort, to explore the correlates for meeting both targets by multivariate analysis, and to examine the barriers and motivations to engage in PA.
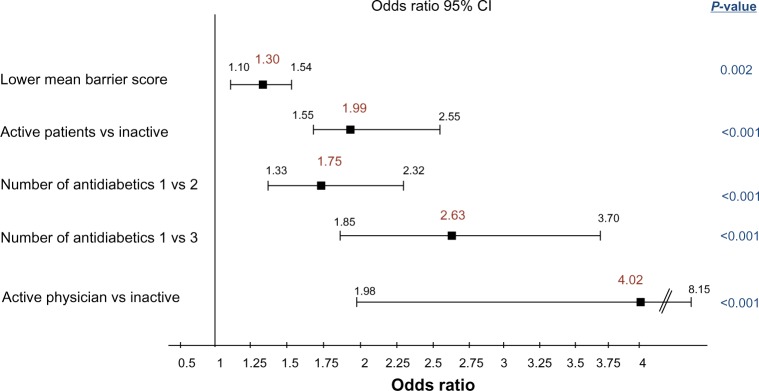
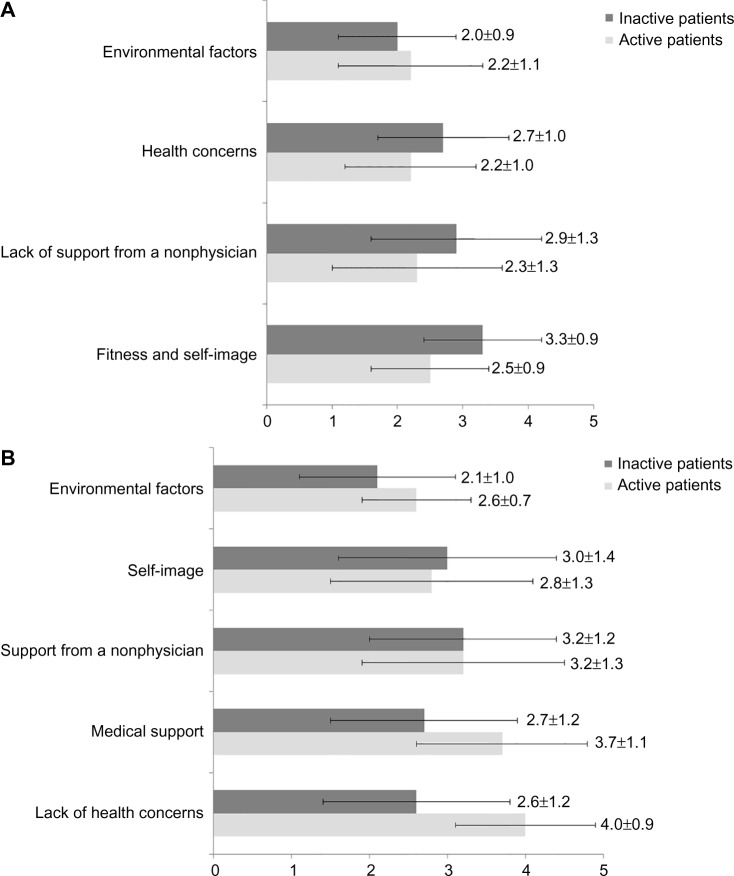
About 1,766 patients were analyzed. Active (n=628) vs. inactive (n=1,138) patients were more often male, younger, less obese, had shorter durations of diabetes, fewer complications and other health issues, such as osteoarticular disorders (P<0.001 for all). Their diabetes and hypertension control was better and obtained despite a lower treatment burden. The biggest difference in PA between the active vs inactive patients was the percentage who declared engaging in regular leisure-type PA (97.9% vs. 9.6%), also reflected in the percentage with vigorous activities in International Physical Activity Questionnaire (59.5% vs. 9.6%). Target control was achieved by 33% of active and 19% of inactive patients (P<0.001). Active patients, those with fewer barriers to PA, with lower treatment burden, and with an active physician, were more likely to reach targets. The physician's role emerged in the motivations (reassurance on health issues, training on hypoglycemia risk, and prescription/monitoring of the PA by the physician). A negative self-image was the highest ranked barrier for the inactive patients, followed by lack of support and medical concerns.
Physicians should consider PA prescription as seriously as any drug prescription, and take into account motivations and barriers to PA to tailor advice to patients' specific needs and reduce their perceived constraints.
尽管体育活动(PA)是2型糖尿病(T2DM)和高血压管理的关键,但在实践中却难以实施。
横断面观察性研究。参与研究的医生被要求招募两名活跃患者和四名不活跃患者,通过里奇 - 加尼翁(RG)自我问卷进行筛查(得分≥16分为活跃)。患者随后完成国际体育活动问卷。目的是评估活跃组与不活跃组患者实现个体化糖化血红蛋白和血压目标(<140/90 mmHg)的情况,通过多变量分析探索达到两个目标的相关因素,并检查参与体育活动的障碍和动机。
共分析了约1766名患者。活跃患者(n = 628)与不活跃患者(n = 1138)相比,男性更多、更年轻、肥胖程度更低、糖尿病病程更短、并发症和其他健康问题更少,如骨关节疾病(所有P<0.001)。他们的糖尿病和高血压控制更好,且治疗负担更低。活跃患者与不活跃患者在体育活动方面的最大差异在于宣称参与定期休闲型体育活动的百分比(97.9%对9.6%),这也反映在国际体育活动问卷中剧烈活动的百分比上(59.5%对9.6%)。33%的活跃患者和19%的不活跃患者实现了目标控制(P<0.001)。活跃患者、体育活动障碍较少、治疗负担较低且有积极医生指导的患者更有可能达到目标。医生的作用体现在动机方面(对健康问题的 reassurance、低血糖风险培训以及医生对体育活动的处方/监测)。消极的自我形象是不活跃患者排名最高的障碍,其次是缺乏支持和医疗方面的担忧。
医生应像对待任何药物处方一样认真考虑体育活动处方,并考虑体育活动的动机和障碍,以便根据患者的具体需求提供建议并减少他们感知到的限制。